
These articles explore the body, the mind, the environment, and the systems that shape human health. Each piece is written to make complex ideas easier to understand, whether the topic is training, nutrition, sleep, stress, digestion, symptoms, physiology, disease, or the way modern life affects how we feel and function.
Strength, Health, & the Art of Living Well
Factors in Non-Contact ACL Injuries
A short animation of typical conditions leading to a non-contact ACL injury.
Pre Workout Supplements: Hypertrophy Priority
Here are some supplement recommendations for athletes seeking to maximize Hypertrophy. With Hypertrophy we are trying to maximize the acidic environment to induce as much damage, cell swelling and hyperemia as possible. What can we take preworkout to help this along?
Primarily, we will want to look at things that shuttle nutrients and blood into the muscle.
- Citruline Malate: reduces fatigue and improves muscle endurance. More effective than Arginine. Arginine actually decreases GH during your workout when taken pre exercise. Arginine is best used before bed.
- Antioxidants : Alpha Lipoic Acid, grape seed extract and CoQ10 improve mitochondrial function and will allow for more blood flow to muscles during training.
- Beet Root Powder: Vasodilator, will induce a pretty gnarly pump.
- Neurotransmitter boosters: these will be important for anyone that has a hard time getting amped up to train. I advise against taking caffeine as a pre workout before Hypertrophy sessions because caffeine is a vaso constrictor. That means that taking caffeine with nutrients to chase the pump is a bit futile. There is a trade off for sure. If training without caffeine leads to a shit workout, then it may be worth your while to take caffeine instead of some of the vasodilators. Taking both at the same time though, to me, is a waste of money.
- BCAAs: provides energy and will prevent muscle protein breakdown during training.
- Creatine: will help sustain energy levels throughout your sessions and get more fluid into the muscles.

Why do partial squats not transfer very well to sport?
By Chris Beardsley, S&C Research columnist
Partial squats make you stronger at partial squats, but do not transfer to full squats. On the other hand, full squats make you stronger at full squats and also make you stronger at partial squats (although usually not quite as well as partial squats).
This is probably because the mechanisms that produce joint angle-specific strength gains are different after training at long muscle lengths, compared to training at short muscle lengths. Training at longer muscle lengths involves more regional hypertrophy, which seems to transfer better to strength across the whole range of motion.
Even so, many coaches have noted that the joint angles in partial squats are similar to the joint angles in the stance phase of running gait, or during jumping. Because of this similarity between joint angles, they suggest that partial squats should transfer better to sport than full squats, as they should produce the greatest gains in strength exactly where we need them.
And this makes a lot of sense.
On the other hand, most research shows that full squats are superior compared to partial squats for improving athletic performance in many respects, particularly jumping.
So what mechanism could be causing this disparity?
What is the background?
You should be able to follow this article without too many problems if you remember that we are normally stronger at one joint angle compared to all the rest, which we call the angle of peak torque.
This angle of peak torque can be changed in different ways, by different types of training.
Training programs using full ranges of motion, using long muscle lengths, or eccentrically all tend to move the angle of peak torque to a joint angle corresponding to a longer muscle-tendon length. In contrast, training programs using a partial range of motion, or short muscle lengths, tend to move the angle of peak torque to a joint angle corresponding to a shorter muscle-tendon length.
And most importantly, changing the angle of peak torque is very likely one of the main mechanisms that causes joint angle-specific gains in strength.
However, angles of peak torque are normally measured using isometric tests, and they might differ during dynamic contractions, particularly at higher speeds.
So does this happen?
Do angles of peak torque differ with angular velocity?
Full range of motion exercises might transfer better to sport than partial range of motion exercises if the angles of peak torque are different when we measure them at different speeds.
This will be particularly relevant if our exercises are traditional, heavy squats, as they involve much slower movement speeds than jumping or sprinting.
And this does happen!
The angle of peak torque is seen at joint angles corresponding to shorter muscle-tendon lengths as angular velocity increases (Moffroid et al. 1969; Knapik et al. 1983; Kannus & Jarvinen, 1991; Yoon et al. 1991; Khalaf et al. 1997; Khalaf et al. 2001; Khalaf & Parnianpour, 2001; Anderson et al. 2007; Ripamonti et al. 2008), although this effect is not always observed consistently in every study, and is much less marked above 180 degrees/s (Frey-Law et al. 2012).
The following charts derived from data reported by Yoon et al. (1991) show how the angle of peak torque alters with increasing angular velocity. Each line represents a different angular velocity moving through the same joint angle range of motion.
Here is knee flexion (contracting from left to right):

As you can see, as the movement speed increases, two things happen.
Firstly, the lines shift downwards, because force reduces as angular velocity increases (because of the force-velocity relationship).
Secondly, the angle of peak torque moves further to the right as angular velocity increases. This means that the angle of peak torque occurs at progressively shorter and shorter muscle-tendon lengths as angular velocity increases.
Here is knee extension (contracting from left to right):

Why do angles of peak torque differ with changing speed?
As you can see from the charts, the angle of peak torque moves to a joint angle that corresponds to shorter and shorter muscle-tendon lengths, with increasing speed.
This probably happens because even though the muscle-tendon lengths are the same at each joint angle, the muscle and tendon do not change length in the same way at different contraction speeds (don’t forget that tendons always lengthen to a greater or lesser extent when a muscle contracts, even when the contraction is purely a concentric contraction that involves a shortening of the muscle-tendon unit).
Fast contractions involve small muscle forces, which cause a smaller amount of tendon elongation at the start of the contraction.
The smaller amount of tendon elongation in fast contractions means that the muscle stays lengthened for longer in the concentric phase of the contraction. This allows the muscle to stay on the plateau of the length-tension curve for longer. Therefore, the angle of peak torque is shifted to much later in the overall joint angle range of motion (Murray et al. 1980).
Slow contractions involve high muscle forces, which cause much more tendon elongation at the start of the contraction.
This greater tendon elongation means that the muscle does not remain lengthened for very long during the concentric contraction. So it drops off the plateau of the length-tension curve quickly. Therefore, the angle of peak torque is seen earlier on in the overall joint angle range of motion (Murray et al. 1980). And isometric contractions are the slowest, strongest contractions of all.
Why is this important?
Why is contraction speed important for the angle of peak torque?
There are two key implications.
Firstly, it means that the angle of peak torque in dynamic movements is always at joint angles corresponding to shorter muscle-tendon lengths compared to the isometric angle of peak torque.
Secondly, it means that sporting movements at very high angular velocities have angles of peak torque at joint angles corresponding to very short muscle-tendon lengths. However, even when measured in the same person, these are not the same angles of peak torque as slower, barbell exercises or isometric tests. Those angles of peak torque occur at much longer muscle-tendon lengths.
This may be why full range of motion heavy resistance training exercises transfer better than similarly-loaded partial range of motion exercises to many high-velocity athletic movements.
What does this mean for jumping?
The quadriceps are key for jumping, and most jumping requires an angle of peak torque at moderate quadriceps lengths, as neither jumpers nor team sports athletes bend their knees down to the levels seen during a full squat before take-off.
This has led some coaches to assume that partial squats might be helpful, as they seem to involve a peak contraction around the same sort of joint angle.
But although this sounds logical, it ignores how the angle of peak torque changes with movement speed.
During a slow, heavy squat, the angle of peak torque will be observed at long muscle lengths. On the other hand, a jump is clearly a very fast movement and so the corresponding angle of peak torque will be at a much shorter muscle length.
If we train at long quadriceps muscle lengths, such as in the deep squat, we shift the angle of peak torque towards a longer muscle length. Because increasing movement speed moves angles of peak torques towards shorter muscle lengths, however, this will correspond to an angle of peak torque at moderate muscle lengths when we measure it at a fast velocity.
This is exactly where we need them for the jump.
If we train at short-to-moderate quadriceps muscle lengths, such as in the partial squat, we shift the angle of peak torque towards a shorter muscle length. Because increasing movement speed moves angles of peak torques towards shorter muscle lengths, however, this will correspond to an angle of peak torque at very short muscle lengths when we measure it at a fast velocity.
This is not where we want them for the jump.
And this is why deep squats transfer much better to jumping than partial squats (Weiss et al. 2000; Hartmann et al. 2012; Bloomquist et al. 2013).
Although there is less research available for sprinting, the same principles will apply.
Conclusions
Some people have proposed that partial squats should transfer better to sport than full squats because of the similar joint angles involved. However, full squats are definitely superior, and this is very clear in relation to jumping.
The reason for this discrepancy is that the angle of peak torque changes with movement speed. The angle of peak torque is found at shorter muscle-tendon lengths when measured at fast speeds, compared to when measured at slow speeds.
This is likely because even though the muscle-tendon lengths are the same at each joint angle, the muscle and tendon do not lengthen to the same extent at different speeds, and the amount of tendon elongation is less during fast contractions, which allows the muscle to remain on its length-tension plateau for longer.
Heavy, slow exercises such as full squats produce peak contractions at long muscle-tendon lengths. Because of differences in the amount that the tendon changes length, these angles of peak torque correspond very well to the peak contractions in athletic movements at joint angles corresponding to shorter muscle-tendon lengths, such as in jumping.
References
- Anderson, D. E., Madigan, M. L., & Nussbaum, M. A. (2007). Maximum voluntary joint torque as a function of joint angle and angular velocity: model development and application to the lower limb.Journal of Biomechanics, 40(14), 3105-3113.
- Bloomquist, K., Langberg, H., Karlsen, S., Madsgaard, S., Boesen, M., & Raastad, T. (2013). Effect of range of motion in heavy load squatting on muscle and tendon adaptations. European Journal of Applied Physiology, 113(8), 2133-2142.
- Frey-Law, L. A., Laake, A., Avin, K. G., Heitsman, J., Marler, T., & Abdel-Malek, K. (2012). Knee and elbow 3d strength surfaces: peak torque-angle-velocity relationships. Journal of Applied Biomechanics, 28(6), 726-737.
- Hartmann, H., Wirth, K., Klusemann, M., Dalic, J., Matuschek, C., & Schmidtbleicher, D. (2012). Influence of squatting depth on jumping performance. Journal of Strength & Conditioning Research, 26(12), 3243.
- Kannus, P., & Jarvinen, M. (1991). Knee Angles of Isokinetic Peak Torques in Normal and Unstable Knee Joints. Isokinetics and Exercise Science, 1(2), 92-98.
- Khalaf, K. A., Parnianpour, M., Sparto, P. J., & Simon, S. R. (1997). Modeling of functional trunk muscle performance: Interfacing ergonomics and spine rehabilitation in response to the ADA.Journal of Rehabilitation Research and Development, 34(4), 459.
- Khalaf, K. A., Parnianpour, M., & Karakostas, T. (2001). Three dimensional surface representation of knee and hip joint torque capability. Biomedical Engineering: Applications, Basis and Communications, 13(02), 53-65.
- Khalaf, K. A., & Parnianpour, M. (2001). A normative database of isokinetic upper-extremity joint strengths: towards the evaluation of dynamic human performance. Biomedical Engineering: Applications, Basis and Communications, 13(02), 79-92.
- Knapik, J. J., Wright, J. E., Mawdsley, R. H., & Braun, J. (1983). Isometric, isotonic, and isokinetic torque variations in four muscle groups through a range of joint motion. Physical Therapy, 63(6), 938-947.
- Moffroid, M., Whipple, R., Hofkosh, J., Lowman, E., & Thistle, H. (1969). A study of isokinetic exercise. Physical Therapy, 49(7), 735.
- Murray, M. P., Gardner, G. M., Mollinger, L. A., & Sepic, S. B. (1980). Strength of Isometric and isokinetic contractions knee muscles of men aged 20 to 86. Physical Therapy, 60(4), 412-419.
- Ripamonti, M., Colin, D., & Rahmani, A. (2008). Torque–velocity and power–velocity relationships during isokinetic trunk flexion and extension. Clinical Biomechanics, 5(23), 520-526.
- Weiss, L. W., Fry, A. C., Wodd, L. E., Relya, G. E., & Melton, C. (2000). Comparative Effects of Deep Versus Shallow Squat and Leg-Press Training on Vertical Jumping Ability and Related Factors. The Journal of Strength & Conditioning Research, 14(3), 241-247.
- Yoon, T. S., Park, D. S., Kang, S. W., Chun, S. I., & Shin, J. S. (1991). Isometric and isokinetic torque curves at the knee joint. Yonsei Medical Journal, 32(1), 33-43.
Is physical strength a virtue?
Judging by the way so many people revere elite athletes, it seems arguable that physical strength is a virtue in the ancient sense of that word, i.e. a human excellence, or an excellence in a human being who possesses it. Or at least it is commonly regarded that way.
That’s controversial enough, but could it even be an excellence with moral or ethical significance? That sounds like a very strange notion to modern ears, but Aristotle would (arguably) have thought so, and the idea can be developed as part of a sophisticated ethical theory that deals with at least the most obvious objections on the ground of absurdity, etc. This would obviously have consequences for current debates about human enhancement technologies.
In the current issue of The Journal of Evolution and Technology, Kyle Oskvig broaches this tricky subject. He does not offer a full defense of Aristotle, but he does show that an evolved, reconstructed version of Aristotelian ethics can make such ideas seem much less crazy than we moderns are inclined to think. Check it out!

Chocolate Milk For Post-Workout: A Look at the Research

Over recent years, there has been a massive initiative to promote chocolate milk as “the best” drink for post-training recovery. Milk advertisers use very high level athletes as spokespersons to sell a product to people who are indeed active, but often very far from the training level of an Olympic athlete.
Nautilus Plus is participating to this initiative: “Whether you are a professional athlete or a weekend sports enthusiast, recover from your next training faster with the Ultimate Chocolate Milk®.”(1) Do we really need to fill ourselves with all this added sugar after our training?
One litre of chocolate milk contains up to 100 to 110 g of sugar!!! The quantity of sugar that the body can absorb is limited. In fact, the sugar will be stored in the liver and muscles in the form of glycogen, which only represents 5 % of the body’s total energy reserves (2). If your objective is, as for the majority of people, to lose fat, you need to remember this: to allow yourself to consume a supplement rich in carbohydrates after your training, you will have to have emptied or seriously depleted your glycogen stores in order for the extra sugar absorbed to be used to renew your glycogen stores. And if you absorb more sugar than you need to renew your reserves, it will be transformed into fat (3).
Scientific studies
Many scientific studies have been done on sports nutrition supplements and some included chocolate milk. The purpose of these studies was to determine which mixture of molecules, and in what proportion, best promotes post-training recovery as well as athletic performance. Almost all these studies followed this particular protocol:
- Study participants were subjected to intense exercise at 70 to 85% of their VO2 max during 1 to 3 hours. The purpose of this step was to considerably reduce the muscle and hepatic glycogen stores since 70 to 80% of the energy spent at 85% VO2 max is derived from glycogen. Under 65% of VO2 max, mostly fatty acids are used (4, 5).
- A recovery period between 4 and 8 hours followed to allow the participants to replenish their glycogen stores with the various sports nutrition supplements covered in the study.
- Participants were then subjected to a second high intensity exercise (VO2 max between 70 and 85%) until exhaustion (loss of 85 to 95% of their hepatic glycogen and 65 to 85 % of their muscle glycogen) (6). The difference in time or distance between the performances will determine which sports nutrition supplements helped the athlete the most to recuperate between the two sessions.
.
The role of these sports nutrition supplements is therefore to replenish as quickly and efficiently as possible the glycogen stores which were SIGNIFICANTLY depleted during the first training, in order to allow a second intense performance within 4 to 8 hours.
This situation is certainly frequent among Olympic athletes or athletes from the Tour de France who train several times per day or several days in a row at extreme intensities, but what about other people? Is chocolate milk a good supplement for “weekend athletes” or people who train leisurely, three of four times per week?
After your leisure strength training?
For a person who does resistance strength training, the glycogen stores will fall by 25 to 40 % after an intense strength training (7 to 12), which is relatively little. The glycogen stores lost during the training will be rebuilt through normal nutrition, WITHOUT ANY SUPPLEMENTS, within 24 hours of the training. However, some people consider it very important to MAXIMIZE the production of lean muscle mass. So the rapid intake of PROTEIN supplements after the training (within 1 hour if possible, up to 3 hours later) is important since it promotes maximum muscle synthesis(13 to 33). Recently, a research team questioned this principle claiming that it would be the total quantity of proteins ingested each day that would prevail over the moment at which they are ingested (34, 35). The same team also mentioned that if a “window” for taking a protein supplement and maximizing the production of lean muscle mass does exist, it would rather span over a 4 to 6 hour period following the strength training.
According to various recent studies, 20 to 25g of proteins would be the recommended amount to take after a resistance training (25, 33, 36). Witard et al., 2014 consider that 20 g of whey protein containing approximately 2 g of leucine optimally stimulates muscle synthesis (33). A litre of chocolate milk contains approximately 30g of proteins, including 80% of micellar casein and 20% of whey (37). Studies on post-training muscle synthesis clearly show the very poor efficiency of micellar casein for this purpose (26, 28, 38, 39, 40) because it precipitates in the stomach and the absorption of amino acids responsible for muscle synthesis is therefore very slow (26, 41, 42, 43). One argument that is often used by chocolate milk advocates is that milk (skim) is more efficient than soy protein or casein to promote muscle synthesis (23, 24). That’s true! It is actually the 20% of whey proteins contained in the milk that makes it efficient for muscle regeneration (26, 28, 40). What they don’t say is that purified whey protein (concentrate or isolate) is the best all around for lean muscle mass gain (26, 28, 40, 44, 45, 37) and, consequently, is better than milk. Whey protein is very rich in BCAA and is quickly absorbed by the intestine, as opposed to casein which is absorbed slowly. Therefore, why take a milk supplement if a whey protein shake is more efficient? Not only does chocolate milk contain large quantities of casein, but it can also contain saturated fat (if it’s full fat) as well as a large quantity of added simple sugars, on top of the lactose. So, is it useful to add all this sugar to the proteins (which are already not optimal) to maximize muscle synthesis after my resistance training?
Some studies show that carbohydrates (CHO) could inhibit muscle breakdown caused by training (10, 46, 47, 48, 49). A few groups claim that a carbohydrate/protein (CHO:PRO) supplement would facilitate a better muscle synthesis since it would inhibit muscle breakdown (15, 32, 46, 48, 50, 51). Nevertheless, some of these studies did not include a control group for the proteins (PRO) only. So it is difficult to evaluate whether adding CHO to PRO provides an advantage or not over PRO taken separately. As for the few studies that included a control group for the PRO, the quantity used was sub-optimal and was given in the form of amino acids (46, 48, 50). However, when a control group taking PRO optimally is included in the study, adding CHO to PRO did not show any advantage in terms of lean muscle mass gain (49, 52 to 57). CHO: PRO ratios used in the studies on resistance training varied between 1:1 and 3:1 whereas chocolate milk offers a ratio between 3:1 and 4:1. That is a lot of unnecessary sugar!
In turn, adding CHO to protein supplements can be necessary when several INTENSIVE resistance trainings are planned during the same day. In such a case, the athlete must quickly renew its glycogen stores (58, 59). To this end, 1g/kg of weight of CHO should be added to the proteins and consumed immediately after the training; moreover, a meal should follow 2 hours after the training (59, 60). So you must weigh at least 220 lbs and must train intensely more than once a day to allow yourself a litre of chocolate milk. Even then, you won’t achieve optimal results because of the casein, which constitutes 80% of the total proteins, and because of the 2:1:0.46 (glucose:fructose:galactose) ratio of the various sugars present in the chocolate milk (61).
The fructose contained in chocolate milk comes from high fructose corn syrup (which has a very bad reputation) and from sucrose (1 glucose +1 fructose). In 2004, Bray GA et al. suggested that the obesity epidemic in the United-States was related to the HFCS found everywhere and in large quantities in our nutrition (62). However, the new report published by The International Journal of Obesity, 2015 (63) suggests that this epidemic cannot be linked to HFCS due to the lack of evidence demonstrating that HFCS would be worse than table sugar (sucrose) (63, 64, 65). Yet, chocolate milk contains both of these additives. The fructose contained in almost equal quantities in both these additives could be linked to obesity (66, 67). Some scientists are reluctant to establish such a link (63, 64). A small quantity of fructose consumed every day, such as normal consumption of fruits, is harmless. Unfortunately, fructose is now added in almost all processed food. So it’s easy to exceed the healthy daily quantities of “natural” fructose. The body metabolises fructose differently from glucose. The liver metabolises 70% of the blood fructose (compared to 15 to 30% for the glucose) (38) and will leave the remaining 30% to the other tissues, namely the kidneys, the testicles, the fatty tissues, the brain and the skeletal muscle (69). So the muscles will absorb a negligible amount of fructose (68). A large consumption of fructose can contribute to the development of the metabolic syndrome, consisting in weight gain, increased resistance to insulin, hypertension, and elevated triglyceride in the blood stream (67, 69). High quantities of fructose are also associated to increased cholesterol, LDL particles and visceral obesity (69).
After an intense cardiovascular training, such as a marathon, when the glycogen stores in the liver are low, the fructose present in a sports nutrition supplement will be used to replenish the hepatic stores. Furthermore, for marathon runners performing at high intensities for a long period of time, the intake of fructose in the form of supplements DURING performance at a ratio of 2:1 (glucose/maltodextrin:fructose), offers a definite advantage because it allows faster absorption of sugars through the intestines since different transporters are used for these two sugars. The supplement would also improve gastro-intestinal comfort and would increase these athletes’ performance (70 to 76). If, however, the quantity of fructose consumed is higher than what is needed to replenish the hepatic stores, the surplus could potentially be converted into fat (66). So for people who do resistance training, consuming fructose is of no value. Conclusion? If you need CHO to perform well during your second strength training, you should add glucose/maltodextrin to your whey proteins, in order to avoid consuming fructose unnecessarily.
Finally, at the beginning of 2015, Stuart M. Phillips’ team established that drinking 500ml of chocolate milk every day (18g of proteins) as a supplement, while following a resistance program three times per week over a period of twelve weeks, has no effect on muscle hypertrophy or on strength gain compared to a control group taking no supplements (77).
What about after leisure endurance training?
Many active people do endurance training several times per week such as jogging, spinning, swimming, etc. for one hour. The extent of the muscle and hepatic glycogen loss will vary according to the effort expended. To consume glycogen as a primary source of energy, the level of effort intensity must reach 70% and must be maintained for an extended period of time (4, 5, 78). Laboratory experiments have shown that glycogen stores decline by 50 to 75% after 3 hours of cycling at 70% of VO2max (79, 80). By increasing the effort to 80% of VO2max, you can continue your activity for 2 hours before running out of glycogen. Another example is that the glycogen stores depletion of marathon runners occurs, for 40% of them, around the 34th kilometre, commonly called “the wall”, when they sustain an effort of approximately 80% of VO2max(81, 82, 83) during more than 2h30. Do you think you will be burning as much glycogen during your hour of spinning?
The glycogen stores lost during the training, even if this loss is significant, will be rebuilt through normal nutrition, WITHOUT ANY SUPPLEMENTS, within 24 hours of the training (84,85). Moreover, the meal frequency will have no incidence if the post-exercise recovery happens over more than 24 hours (85, 86, 87). It is unnecessary for someone coming out of an hour of spinning or jogging to ingest all the added sugars contained in chocolate milk since the subsequent meals will contain sufficient carbohydrates (CHO) to replenish the poorly depleted glycogen stores. Therefore, the person will be ready for the next training a few days later.
Without being Olympic athletes, some people will train intensely and frequently during a week. In such case, the quantity of CHO these people consume every day must be adjusted, spread throughout their meals according to the frequency and intensity of their training. Burke et al. 2011 recommend to take a quantity of CHO every day, depending on the type of training performed (intensity and duration) to allow for a good glycogen resynthesis during the 24 hours following the training (88).
If the objectives of the person doing endurance training don’t include maximum muscular development, the muscle regeneration following an effort, namely the replenishment of glycogen stores, will occur normally with the proteins contained in the subsequent meal, when taken in sufficient quantity.
Supplements are necessary when training sessions are very intense and close together (a few hours) and require to quickly replenish the glycogen stores (in less than 24 hours).
What about high level athletes? (1.3% of the American population are athletes and of which 0.006% are professional athletes) (89).
Although chocolate milk is not intended for Olympic athletes, choosing such athletes as spokesperson to promote chocolate milk as a post-training supplement is almost an obligation; indeed, practically only these athletes could ultimately use chocolate milk as a sports nutrition supplement. Moreover, most studies carried out on the subject are done in a top level training context. But is chocolate milk, as alleged by the television commercials, a good choice for this 1% of the population ?
The purpose of a supplement is to promote fast recovery between two trainings done very close together, mainly by QUICKLY regenerating the glycogen stores. So the muscle glycogen resynthesis speed is important. It was established that this synthesis is faster when CHO are taken right after the training (90, 91, 92) and can be maintained during 6 hours with frequent intake of this supplement (69, 90, 93). Delaying the intake of CHO by 2 hours decreases the resynthesis speed by 50% (16,90). This is particularly important for a fast recovery but is unnecessary for recovery over 24 hours or more (87). OPTIMALLY, the quantity of CHO should be 1.0 to 1.2g/kg of weight/h (94, 95, 96), consumed at 15 to 30 min intervals (97). At this volume and frequency, CHO alone are sufficient to ensure an optimal glycogen synthesis. Sure! But chocolate milk doesn’t only contain CHO!
Is it useful to add proteins to CHO? (98)
To determine which supplement is the best one, we need to compare the different supplements. It is difficult to compare the studies that analyze the effect of adding proteins to a CHO supplement because several variables differ: 1) intensity (% of VO2max) and duration of the first exercise that aims at reducing the glycogen stores 2) choice of exercise (jogging or cycling) 3) various types of supplements consumed (isocaloric or not, as well as the chosen sugars and proteins) 4) control groups used (lack of placebo or other control groups) 5) carbohydrates:protein ratios (CHO:PRO) will vary between 2:1 (Berardi et al. 2006/2008) (99, 100) and 6.2:1 (Betts et al. 2005) (101) 6) duration and intensity of the second performance (% of VO2max).
Nonetheless, it’s possible to draw certain conclusions.
1: Importantly, the drinks studied must be isocaloric (must contain the same amount of calories) :
Some studies show a performance improvement post-recovery when proteins (PRO) are added to CHO versus a control group taking only CHO (102 to 105). However, the quantity of calories between the two drinks was not adjusted, so it wasn’t possible to determine if the performance improvement could be attributed to the addition of proteins or to the aaddition of energy.
2: It is important to compare the CHO+PRO supplement to a control group taking CHO optimally (1.0 to 1.2g/kg of weight/h) AND which is isocaloric:
Some studies show that the addition of proteins to the CHO supplement improves the second performance when compared to a control group taking a CHO only supplement. But this supplement was given sub-optimally during recovery (96, 102, 104, 106, 107). When the control group took the CHO supplement OPTIMALLY, the studies did not show any improvement in the second performance when proteins were added to the mix, even with variable ratios. (95, 96, 101 to 115, 116). A study showed, however, an advantage (100) (see the “Ratio” section).
So the athlete can chose between taking a mix of CHO + PRO, when it is impossible to optimally take a CHO supplement during recovery (1.2g/kg/h every 30 min during 3 to 4 hours) (94, 95, 96, 117). This indeed makes for a lot of CHO to ingest. But at which ratio must the athlete take its proteins?
3: Ratio
Advocates of chocolate milk allege that a ratio of 4:1 is best to support athletic recovery. This belief comes from one of the early studies done on the subject and which showed that a sports nutrition supplement, Endurox R4, containing 4:1 CHO: PRO offered a performance advantage when compared to a control group taking CHO, namely Gatorade (102). However, Endurox R4 contained two and a half times more CHO than Gatorade, in addition to the whey proteins, which gave it almost four times more calories than the Gatorade supplement consumed SUB-OPTIMALLY by the participants. It is obvious that in these conditions, Endurox R4 improved performance compared to Gatorade given the significant difference in CHO and energy consumed between the two drinks. Since the ratio used in this study was 4:1, which is the same as the chocolate milk ratio, the dairy industry took the opportunity to pretend it was the best ratio. Nonetheless, research continued and more recent studies show that ratios containing less sugar are as efficient, if not more, than a 4:1 ratio. Berardi et al. 2008 show an advantage on the second performance with the CHO: PRO mix at a ratio of 2:1 (CHO: 0.8kg/kg/hand PRO: 0.4kg/kg/h), over the control group taking the CHO supplement optimally (100, 117). So why add more sugar than necessary with a ratio of 4:1 if it offers no advantage?
Studies done on chocolate milk (McLellan TM et al. 2014 (98)) :
There are 5 major studies comparing chocolate milk to a few other sports drinks during a short term recovery between two performances. (118, 119, 120, 121, 122)
- None of these 5 studies explained how the chocolate milk taste was reproduced for the control groups. If the athletes know which type of supplement they are given, it can certainly influence the results; in such a case, the study is no longer “blind”.
- Some studies did not include a placebo or a sub-optimal CHO supplement for the control group (118, 122).
- 4 studies on 5 did not administer the supplement optimally (118, 119, 120, 121). The fifth study did so for the first recovery hour only (122).
- Pritchett et al. 2009 show that chocolate milk (3.8:1) offers no advantage for the second performance over Endurox R4 (3.8:1, isocaloric and same quantity of CHO) (118).
- The other four studies indicated that chocolate milk presented an advantage for the second performance compared to the other drinks studied (119, 120, 121, 122). On the other hand, the studies also present other shortfalls:
For Karp et al. 2006 and Thomas et al. 2009, the glycogen stores reduction protocol was not standardized during the first training(119, 120). That means that the energy expenditure varies a lot from one person to another, even for each individual, from one training session to another. So some groups used more glycogen than others before starting the recovery phase. For Karp et al. 2006 for example, (similar to Thomas et al. 2009), the chocolate milk group (60.8 min) had trained 16% less than the CHO + PRO control group taking Endurox R4 (72.6 min), but equally to the Gatorade group (sub-optimal). These differences can explain the superior performance of the chocolate milk group during the second training. Furthermore, we must report that the study by Karp et al. 2006 was partly financed by the Dairy and Nutrition Council Inc (119).
In the study by Lunn et al. 2012, chocolate milk is compared to a control group taking CHO optimally during the first hour of recovery (122). Despite the fact that the regeneration of the glycogen stores was equal between the two groups, the performance of the chocolate milk group was superior to that of the CHO control group during the second performance (difference of a few seconds). However, the intensity of the second performance was at 100% VO2max and lasted a very short time (203 vs 250 sec). In these very high intensity and very short duration conditions, the more or less important level of muscle glycogen stores before the effort don’t seem to influence performance (123, 124, 125, 126), as opposed to a lower intensity and longer duration performance. So optimally replenishing the glycogen stores is probably not that important in this case. Even the authors admit that the type of test used and the inability to mask the taste of the chocolate milk may have influenced the results. The authors challenge this by emphasizing that the purpose of their study was to show that chocolate milk promotes a better muscle synthesis compared to CHO alone (122). Milk contains proteins whereas the CHO of the control group contained none. So it is not surprising that the results show that chocolate milk increases muscle synthesis. A control group also taking proteins would have certainly given results similar to the chocolate milk, and possibly even better results if whey protein would have been used.
The study by Furguson-Stegall et al. 2011 compared a chocolate milk ratio smaller than 3:1 to an isocaloric CHO drink and to a placebo (water) (121). The drinks were given sub-optimally. The performance of the chocolate milk group was superior by a few minutes during the second training (40km of cycling) compared to the CHO control group. Nonetheless, the glycogen resynthesis was better with the CHO control group, a result that is slightly contradictory. This study was financed by a Chair established by The National Dairy Council, as well as The National Fluid Milk Processor Promotion Board.
Therefore, the contradictory results, the lack of control groups, the questionable protocols and the inability to obtain blinded studies, do not allow to claim without any doubt that chocolate milk is the best supplement compared to the other supplements studied. The number of serious studies on chocolate milk will have to be considerably larger. Furthermore, these studies will have to be done more independently (not financed by the dairy industry, for example) to achieve more conclusive results.
It should be noted that chocolate milk has not been compared to a supplement offering a ratio of 2:1 previously shown to offer better performances than a CHO supplement taken optimally by Berardi et al. 2008 (100). For comparison purposes, a 200lbs (90kg) man who ingests a supplement offering a ratio of 2:1 will consume 72g of CHO/h instead of 85g/h for a chocolate milk supplement taken optimally. So this represents approximately 40g less of added sugar consumed, during a 3 hour recovery, to achieve the same result, if not better.
The composition of the supplement used by Berardi et al. 2008 is also very different from that of chocolate milk; it contained 33% of maltodextrin, 33% of glucose and 33% of whey (100). So in addition to the ratio, the choice of nutrients is important.
4: CHO
Maltodextrin (MD) seems to be the ideal sugar for muscle glycogen resynthesis after an intense effort. Piehl-Aulin et al. 2000 have shown that a supplement containing very high molecular weight polyglucosides such as maltodextrin would be 25% more efficient for muscle glycogen synthesis than a low molecular weight glucose, maltose or oligomer supplement (127). This would be due to the faster absorption rate of sugars by the intestines, as well as an increased rate of gastric emptying. As seen previously, while the addition of fructose to MD (ratio 2:1, MD: FRU) represents a major advantage DURING a long performance (more than 2h30) such as a marathon(128), it seems that for the rapid muscle glycogen resynthesis between two performances, the addition of fructose or galactose to MD offers no advantage (129). Regarding sucrose (glucose: fructose), no advantage was observed concerning glycogen resynthesis when compared to glucose alone (69, 129, 130, 131, 132), nor during the second performance (129 to 131). Again, we notice that the fructose and galactose portion found in chocolate milk is not useful for the post-training recovery.
5: Proteins
As for strength training, the type of proteins added to the CHO as a post-training supplement is important. However, few studies compare the different types of proteins and their effects on the glycogen resynthesis speed during a short term recovery. Morifuji et al. 2010 have shown, in rats, that adding whey hydrolysate to CHO is more efficient for glycogen synthesis than the CHO control group, followed by non-hydrolysed whey and BCAA. Casein ranked dead last, having no significant effect on glycogen synthesis compared to the intake of glucose alone (133). A large proportion of studies on athletic recovery used hydrolysed or non-hydrolysed whey protein isolate as a source of proteins in their mixes. The advantage over the chocolate milk proteins (mainly consisting of casein) is that in addition to being absorbed faster, the whey protein allows a higher protein concentration mix while restricting the volume to be consumed. It is a non-negligible advantage for the athletes as well as for achieving ratios of 2:1, for example.
Lactose
Milk contains 25g of lactose per 500ml. The capacity to break down lactose into glucose and galactose molecules depends on the presence of the lactase enzyme in the small intestine. “Normally” in humans, the presence or activity of lactase is very strong at the beginning of childhood and starts declining after the child is weaned until it almost disappears in adulthood. The person is then unable to digest lactose for the rest of his or her life (134, 135, 136). Between 65 and 70% of the world population is unable to digest lactose once they reach adulthood (137, 138). So only 30 to 35% of the population can actually digest lactose. Why? During the human evolution, four different mutations occurred, namely a major one that occurred in Europe, which kept the lactase gene active and thus allowing some Caucasians to digest lactose during all their life(137 to 139). These European Caucasians travelled, reached America and gave their descendants the possibility to also carry this mutation. Despite this, approximately 21% of North Americans who have problems digesting lactose are Caucasians (140). The ability to digest lactose is directly linked to the quantity of lactase produced by the intestine (134 to 136) and this quantity varies from one person to another. So some people have more difficulty than others to digest this sugar even though it may not be a true intolerance, rather an incomplete digestion that can sometimes be asymptomatic (140 to 143).
Making up 50% of the sugar contained in chocolate milk, we must seriously question the lactose digestion capacity to quickly regenerate the glycogen stores post-training, if we take into account the differences in the quantities of lactase present in the intestines of each individuals. It was shown that adding sugar (144, 145, 146, 147), fat (147) or chocolate (144, 145) in milk slows down the digestion process. This slowing down certainly promotes a better digestion of the lactose by the lactase present in various amounts, but does make digestion more efficient ? Since it can be very difficult for some people, around the world, to digest lactose, chocolate milk could only be used by a very small portion of athletes, which already represent a tiny portion of the population.
Who promotes chocolate milk?
Besides dairy producers in Quebec and Canada, many nutritionists promote chocolate milk as an ideal post-training supplement. The most relevant comment made to this effect by a nutritionist is the comment from Isabelle Charêt, coach and triple medallist in speed skating at the 1994, 1998 and 2002 winter Olympics (148). She says that chocolate milk would be a lot more useful to people who train intensively: “Someone who goes to the gym three times a week has plenty of time to recover. But I still recommend to drink chocolate milk because people in general don’t drink enough milk.” Ah! But that’s the issue! We have to drink milk!
I will not go into further detail on this subject, but very recently (2013), a team from Harvard University acknowledged publicly the need to decrease to less than two portions per day, or to stop all together, our milk consumption (149, 150). The powerful dairy industry lobby, which represents a third of Quebec’s agriculture and 5 billion dollars of Canadian GDP, imposed itself to maintain the dominant position dairy products hold in the Canadian food guide (151). Nonetheless, the following question remains: is it necessary to include chocolate milk in our diet? Many scientists seem to think that it’s not (149, 150, 151, 152).
Conscious of the extent of the damages caused by the overconsumption of added sugars to human health, how can we encourage the consumption of such sugars just to impose a supplement that is increasingly considered as unnecessary to our health?
Conclusion? If you enjoy a glass of chocolate milk once in a while, as a treat, it’s no big deal! But if milk commercials encourage you to drink one after each of your trainings, and you are not an Olympic athlete (and even then…), I hope you’ll think twice about it.
You know the saying: When it seems too good to be true…
References :
1. http://www.nautilusplus.com/courriel/e-magazine/avril2011/pdf/Chronique_Saputo_fr.pdf
2. McArdle W, Katch, F & Katch. V. (2001). Carbohydrates, lipids, and proteins. In P. Darcy (Ed.), Exercise physiology (Vol. 5, pp. 11-13). Baltimore, MD: Lippincou Williams & Wilkins.
3. Charkas A & Golota S. (2014). An intermittent exhaustion of the pool of glycogen in the human organism as a simple universal health promoting mechanism. Medical hypotheses. 82 : 387-389
4. Romijn JA, Coyle EF, Sidossis et al. (1993). Regulation of endogenous fat and carbohydrate metabolism in relation to exercise intensity and duration. Am J Physiol Endocrinol Metab. 265, E380-E391.
5. Holloszy JO & Hohrt WM. Regulation of carbohydrate and fat metabolism during and after exercise. Annu Rev Nutr. 16, 121-138. 1996
6. Gregory Tardie, Ph.D. U.S. Sports Academy in Sports Coaching, Sports Exercise Science, Sports Studies and Sports Psychology. http://thesportjournal.org/article/glycogen-replenishment-after-exhaustive-exercise/
7. Tesch PA, Colliander EB, Kaiser P. (1986). Muscle metabolism during intense, heavy-resistance exercise. Eur J Appl Physiol Occup Physiol. 55(4) :362-6
8. Essen-Gustavsson B, Tesch PA. (1990). Glycogen and triglyceride utilization in relation to muscle metabolic characteristics in men performing heavy-resistance exercise. Eur J Appl Physiol Occup Physiol. 61(1-2) :5-10.
9. Robergs RA, Pearson DR, Costill DL et al. (1991). Muscle glycogenolyse during differing intensities of weight-resistance exercise. J Appl Physiol. 70(4) :1700-1706.
10. Roy BD, Tarnopolsky MA, MacDougall JD et al. (1997). Effect of glucose supplement timing on protein metabolism after resistance training. J Appl Physiol. 82 :1882-1888
11. MacDougall JD, Ray S, McCartney N, et al. (1999). Muscle substrate utilization and lactate production during weight lifting. Can J Appl Physiol. 24(3) :209-215.
12. Haff GG, Koch AJ, Potteiger JA, Kuphal KE, et al. (2000). Carbohydrate supplementation attenuates muscle glycogen loss during acute bouts of resistance exercise. Int J Sport Nutr Exerc Metab. 10 : 326-339.
13. Phillips SM, Tipton KD, Aarsland A et al. (1997). Mixed muscle protein synthesis and breakdown after resistance exercise in human. Am J Physiol. 273 :E99-E107.
14. Tipton KD, Ferrando AA, Phillips SM et al. (1999). Postexercise net protein synthesis in human muscle from orally administered amino acids. Am J Physiol. 276 : E628-E634.
15. Rasmussen BB, Tipon KD, Miller SE, Wolf RR. (2000). An oral essential amino acid-carbohydrate supplement enhances muscle protein anabolism after resistance exercise. J Appl Physiol. 88 :386-392.
16. Levenhagen DK, Gresham JD, Carlson MG et al (2001). Post-exercise nutrient intake timing in humans is critical to recovery of leg glucose and protein homeostasis. Am J Physiol Endocrinol Metab. 280, E982-E993
17. Esmarck B, Andersen JL, Olsen S et al. (2001). Timing of postexercise protein intake is important for muscle hypertrophy with resistance training in elderly humans. J Physiol. 15 :535 :301-11
18. Tipton KD, Rasmussen BB, Miller SL et al. (2001). Timing of amino acid-carbohydrate ingestion alters anabolic response of muscle to resistance exercise. Am J Physiol Endocrinol Metab. 281 : E197-E206
19. Borsheim E, Tipton KD, Wolf SE, Wolfe RR(2002). Essential amino acid and muscle protein recovery from resistance exercise. Am J Physiol Endocrinol Metab. 283 :48-57
20. Lemon PW, Berardi JM, Noreen EE. (2002). The role of protein and amino acid supplements in the athlete’s diet : does timing of ingestion matter ? Curr Sport Med Rep. 1(4) :214-221.
21. Volek JS. (2004). Influence of nutrition on responses to resistance training. Med Sci Sports Exer. 36 :689-96
22. Cribb PJ, Hayes A. (2006). Effect of supplement timing and resistance exercise on skeletal muscle hypertrophy. Med Sci Sport Exerc. 38 :1918-1925.
23. Wilkinson S, Tarnopolsky M, MacDonald M, et al. (2007). Consumption of fluid skim milk promotes greater muscle protein accretion after resistance exercise than does consumption of an isonitrogenous and isoenergetic soy-protein beverage. Am J Clin Nutr. 85 (4) :1031-40
24. Hartman J, Tang JE, Wilkinson S, Tarnopolsky M, et al. (2007). Consumption of fat-free fluid milk after resistance exercise promotes greater lean mass accretion than does consumption of soy or carbohydrate in young, novice, male, weightlifters. Am J Clin Nutr. 86 (2) :373-81
25. Moore DR, Robinson MJ, Fry JL, Tang JE, et al.(2009). Ingested protein dose response of muscle and albumin protein synthesis after resistance exercise in young men. Am J Clin Nutr. 89(1):161-8.
26. Tang JE, Moore DR, Kujbida G, Tarnopolsky M, Phillips S. (2009). Ingestion of whey hydrolysate, casein, or soy protein isolate : effect on mixed muscle protein synthesis at rest and following resistance exercise in young men. J Appl Physiol .107(3) :987-92.
27. West DW, Burd NA, Coffey VG et al. (2011) Rapid aminoacidemia enhances myofibrillar protein synthesis and anabolic intramuscular signalling responses after resistance exercise. Am J Clin Nutr. 94 : 795-803.
28. Burd N, Yan Y, Moore DR, Tang JE, et al. (2012). Greater stimulation of myofibrillar protein synthesis with ingestion of whey protein isolate v. micellar casein at rest and after resistance exercise in eldery men. Br J Nutr. 108 :958-62.
29. Churchward-Venne TA, Burd NA, Mitchell CJ, West DW, et al. (2012). Supplementation of a suboptimal protein dose with leucine or essential amino acids: effects on myofibrillar protein synthesis at rest and following resistance exercise in men. J Physiol. 1;590(Pt 11):2751-65.
30. Churchward-Venn TA, Burd NA, Phillips SM et al. (2012). Nutritional regulation of muscle protein synthesis with resistance exercise : strategies to enhance anabolism. Nutr Metab. 9 :40.
31. Tipton KD, Phillips SM. (2013). Dietary protein for muscle hypertrophy. Nestlé Nutr Inst Workshop Ser. Vol 76 :73-84
32. Mori H. (2014). Effect of timing of protein and carbohydrate intake after resistance exercise on nitrogen balance in trained and untrained young men. J Physiol Anthropol. 33 :24
33. Witard OC, Jackman SR, Breen L, et al. (2014). Myofibrillar muscle protein synthesis rates subsequent to a meal in response to increasing doses of whey protein at rest and after resistance exercise. Am J Clin Nutr. 99(1):86-95
34. Schoenfeld BJ, Aragon AA Krieger JW. (2013). The effect of protein timing on muscle strength and hypertrophy : a meta-analysis. J Int Soc Sports Nutr. 10(1):53.
35. Aragon AA, Schoenfeld BJ. (2013) Nutrient timing revisited : is there a post-exercise anabolic window ? J Int Soc Sports Nutr. 10 (1):10-15.
36. Churchward-Venne T, Breen L, Di Donato D et al. (2014). Leucine supplementation of a low protein mixed macronutriment beverage enhances myofibrillar protein synthesis in young men : a double-blind, randomized trial. Am J Clin Nutr. 99(2) :276-86.
37. Devries MC & Phillips SM. (2015). Supplemental protein in support of muscle mass and health : Advantage Whey. Journal of Food Science. Vol 80, S1.
38. Cribb PJ, Williams AD, Hayes A, Carey MF. (2006). The effect of whey isolate on strength, body composition and plasma glutamine. Int J Sport Nutr exer Metab. 16 :494-509.
39. Koopman R., Crombach N., Gijsen, A.P., Walrand, S et al. (2009). Ingestion of a protein hydrolysate is accompanied by an accelerated in vivo digestion and absorption rate when compared with its intact protein. Am J Clin Nutr. 90. 106-115.
40. Penning B, Boirie Y, Senden J, Gijsen A, Kuipers H, van Loon L. (2011). Whey protein stimulates postprandial muscle protein accretion more effectively than do casein and casein hydrolysate in older man. Am J Clin Nutr. 93(5) :997-1005
41. Boirie Y, Dangin M, Gachon P, Vasson M, et al. (1997). Slow and fast dietary proteins differently modulate postprandial protein accretion. Proc Nath Acad, Sci USA. 94 :14930-5.
42. Mahe S, Roos N, Benamouzig R, Davin, L, et al. (1996). Gastrojejunal kinetics and the digestion of [15N]beta-lactoglobulin and casein in humans: the influence of the nature and quantity of the protein. Am J Clin Nutr. 63: 546–552.
43. Bos C, Metges CG, C, Petzke K, et al. (2003). Postprandial kinetics of dietary amino acids are the main determinant of their metabolism after soy or milk protein ingestion in humans. J Nutr. 133 :1308-15
44. Yang Y, Churchward-Venn T, Burd N, Breen L, et al. (2012). Myofibrillar protein synthesis following ingestion of soy protein isolate at rest and after resistance exercise in elderly men. Nutr Metab. (Lond) 9 :57
45. Volek JS, Volk BM, Gómez AL, et al. (2013). Whey protein supplementation during resistance training augments lean body mass. J Am Coll Nutr. 32(2):122-35
46. Miller SL, Tipton KD, Chinkes DL et al. (2003) Independent and combined effect of amino acids and glucose after resistance exercise. Med. Sci Sports Exerc. (35); 3 :449-455
47. Børsheim E, Cree MG, Tipton KD, et al. (2004) Effect of carbohydrate intake on net muscle protein synthesis during recovery from resistance exercise. J Appl Physiol. (1985). 96(2): 674-8.
48. Bird SP, Tarpenning KM, Marino FE. (2006). Independent and combined effects of liquid carbohydrate/essential amino acid ingestion on hormonal and muscular adaptations following resistance training in untrained men. Eur J Appl Physiol. 97(2) :225-38.
49. Glynn EL, Fry CS, Drummond MJ et al. (2010). Muscle protein break-down has a minor role in the protein anabolic response to essential amino acid and carbohydrate intake following resistance exercise. Am J Physiol. 299 : R533-40.
50. Rasmussen BB, Phillips SM. (2003). Contractile and nutritional regulation of human muscle growth. Exerc Sport Sci Rev. 31 :127-131.
51. Borsheim E, Aarsland A, Wolfe RR. (2004). Effect of an amino acid, protein, and carbohydrate mixture on net muscle protein balance after resistance exercise. Int J Sport Nutr Exerc Metab. Jun;14(3):255-71.
52. Cribb PJ, Williams AD, Hayes A. (2007). Creatine-protein-carbohydrate supplement enhance response to resistance training. Med Sci Sport Exerc. 39 :1960-8.
53. Koopman R, Beelen M, Stellingwerff T, Pennings B, et al. (2007). Coingestion of carbohydrate with protein does not further augment postexercise muscle protein synthesis. Am J Physiol Endocrinol Metab. 293(3) :E833-E842.
54. Staples AW, Burd NA, West DW, Currie KD, et al. (2011). Carbohydrate does not augment exercise-induced protein accretion versus protein alone. Med Sci Sports Exerc. 43(7) :1154-1161.
55. Glynn EL, Fry CS, Timmerman KL, Drummond MJ, Volpi E, Rasmussen BB. (2013). Addition of carbohydrate or alanine to an essential amino acid mixture does not enhance skeletal muscle protein anabolism. J Nutr. 143(3) :307-314.
56. Gorissen SHM, Burd NA, Henrike M et al. (2014). Carbohydrate coingestion delays dietary protein digestion and absorption but does not modulate prostprandial muscle protein accretion. J Clin Endocrinol Metab. 99(6) :2250-2258.
57. Pasiakos SM, McLellan TM, Lieberman HR. (2015). The effects of protein supplements on muscle mass, strength, and aerobic and anaerobic power in healthy adults : A systematics review. Sports Med. 45 :111-131.
58. Pascoe DD, Costill DL, Fink WJ et al. (1993). Glycogen resynthesis in skeletal muscle following resistive exercise, Med Sci Sports Exerc. 25 :349-354.
59. Roy BD, Tarnopolsky. (1998). Influence of different macronutrient intakes on muscle glycogen resynthesis after resistance exercise. J Appl Physiol. 72 :1854-1859.
60. Ivy JL, Ferguson LM. (2010). Optimizing Resistance exercise Adaptations through the timing of post-exercise Carbohydrate-protein supplementation. Strength and Conditioning Journal. Vol 32, No1, 30-36.
61. http://voluntocracy.org/Fructose/
62. Bray GA, Nielsen SJ, Popkin BM. (2004). Consumption of high-fructose corn syrup in beverages may play a role in the epidemic of obesity. Am J Clin Nutr. 79(4):537-43.
63. White JS , Hobbs LJand Fernandez S. (2015). Fructose content and composition of commercial HFCS-sweetened carbonated beverages. International Journal of Obesity. 39, 176–182
64. Moeller SM, Fryhofer SA, Osbahr AJ 3rd,et al. (2009). The effect of high fructose syrup. J Am Coll Nutr. 28(6) :619-626
65. White JS. (2008). Straight talk about high-fructose corn syrup : what it is and what it ain’t. Am J Clin Nutr. 88 (suppl) :1716S-21S.
66. Parks EJ, Skojan LE, Timlin MT et al. (2008). Dietary sugars stimulate fatty acid synthesis in adults. J Nutr. 138 :1039-46.
67. Tappy L, Lê KA, Tran C, Paquot N. (2010) Fructose and metabolic diseases : New finding, new questions. Nutrition. 26 : 1044-1049.
68. Kolderup A & Svihus B (2015). Fructose Metabolism and Relation to Atherosclerosis, Type 2 Diabetes, and Obesity. Journal of Nutrition and Metabolism. 1-12
69. Charrez B, Qiao L and Hebbard L. (2015) The role of fructose in metabolism and cancer. Horm Mol Biol Clin Invest. 22(2): 79–89
70. Jentjens RL, Moseley L, Waring RH et al. (2004). Oxidation of combined ingestion of glucose and fructose during exercise. J Appl Physiol. 96 :1277-1284.
71. Jeukendrup AE, moseley L, Mainwaring GI et al. (2006). Exogenus carbohydrate oxidation during ultra endurance exercise. J Appl Physiol. 100 :1134-41.
72. Rowlands DS, Thorburn MS, Thorp RM et al. (2008). Effect of graded fructose coingestion with maltodextrine on exogenous 14C-fructose and 13C-glucose oxidation efficiency and high-intensity cycling performance. J Appl Physiol. 104 :1709-1719.
73. Currell K & Jeukendrup AE. (2008). Superior endurance performance with ingestion of multiple transportable carbohydrates. Med Sci Sports Exerc. 40 :275-281.
74. O’Brien WJ, Rowlands DS. (2011). Fructose-maltodextrin ratio in a carbohydrate-electrolyte solution differentially affects exogenous carbohydrate oxidation rate, gut comfort, and performance. Am J Physiol Gastrintest Liver Physiol. 300: G181-G189
75. Jeukendrup AE. (2013). Multiple transportable carbohydrates and their benefits. Sports Sci Exchange. 26 (108) : 1-5
76. Robert JD, Tarpey MD, Kass LS, et al. (2014). Assessing a commercially available sports drink on exogenous carbohydrate oxidation, fluid delivery and sustained exercise performance. Journal International Society Sports Nutrition. 11 ;8 : 1-14
77. Mitchell CJ, Oikawa SY, Ogborn DI, Nates NJ, et al. (2015). Daily chocolate milk consumption does not enhance the effect of resistance training in young and old man : a randomized controlled trial. Appl. Physiol. Nutr. Metab. 40 : 1-4
78. Hultman E & Sjöholm H. (1983). Energy metabolism and contraction force of human skeletal muscle in situ during electrical stimulation. J Physiol. 345 : 525-32
79. Bosch AN, Dennis SC & Noakes TD (1994). Influence of carbohydrate ingestion on fuel substrate turnover and oxidation during prolonged exercise. Journal of Applied Physiology (Bethesda, Md.), 76(6). 2364-2372.
80. Bosch AN, Weltan SM, Dennis SC & Noakes TD. ( 1996). Fuel substrate turnover and oxidation and glycogen sparing with carbohydrate ingestion in non-carbohydrate- loaded cyclists. Pflugers Archiv. 432(6), 1003-1010.
81. Buman MP, Brewer BW, Cornelius AE et al. (2008). Hitting the wall in the marathon : Phenomenological characteristics and associations with expectancy, gender, and running history. Psychol Sports Exerc. 9 :177-190.
82. Buman MP, Brewer BW, Cornelius AE. (2009). A discrete-time hazard model of hitting the wall in recreational marathon runners. Psychol Sports Exerc. 10 :662-666.
83. Rapoport BI. (2010). Metabolic factors limiting performance in marathon runners. PLOS Computational Biology. 6: 10: 1-13.
84. Burke LM, Collier GR, Beasley SK, et al. (1995). Effect of coingestion of fat and protein with carbohydrate feeding on muscle glycogen storage. J Appl Physiol (1985). 78(6):2187-2192.
85. Costill DL, Sherman WM, Fink WJ et al. (1981). The role of dietary carbohydrate in muscle glycogen resynthesis after strenuous running. Am J Clin Nutr. 34 :1831-36.
86. Burke LM, Collier GR, Davis PG et al. (1996). Muscle glycogen storage after prolonged exercise : effect of the frequency of carbohydrate feedings. Am J Clin Nutr. 64 :115-119.
87. Parkin JAM, Carey MF, Martin IK et al. (1997). Muscle glycogen storage following prolonged exercise : effect of timing of ingestion of high glycemic index food. Med Sci Sports Exerc. 29 :220-224.
88. Burke LM, Hawley JA, Wong SH, et al. (2011). Carbohydrates for training and competition. J Sports Sci. 29(suppl. 1), S17-S27.
89. http://www.answers.com/Q/What_percentage_of_the_US_population_are_professional_athletes,
90. Ivy JL, Katz AL, Cutler CL et al. (1998). Muscle glycogen synthesis after exercise : Effect of time of carbohydrate ingestion. J Appl Physiol. 64,1480-1458.
91. Price TB, Rothman DL, Taylor R et al. (1994), Human muscle glycogen resynthesis after exercise : insulin-dependent and –independent phases. J Appl Physiol. 76, 104-111.
92. Fallowfield JL, Williams C, Singh R. (1995). The influence of ingesting a carbohydrate-electrolyte beverage during 4h of recovery on subsequent endurance capacity. Int J Sport Nutr Exerc Metab. 5 :285-99
93. Ivy JL, Lee MC, Brozinick JT et al. (1988). Muscle glycogen storage after different amount of carbohydrate ingestion. J Appl Physiol. 65, 2018-2023
94. Ivy JI. (2001). Dietary strategies to promote glycogen synthesis after exercise. Can J Appl Physiol. 26(Suppl.) S236-S245.
95. Jentjens RL, van Loon LJ, Mann CH et al. (2001) Addition of protein and amino acids to carbohydrate does not enhance postexercise muscle glycogen synthesis. J Appl Physiol. 91,839-846.
96. van Loon LJ, Saris WH, Kruijshoop M, et al. (2000) Maximazing postexercise glycogen synthesis : carbohydrate supplementation and the application of amino acids or protein hydrolysate mixtures. Am J Clin Nutr. 72, 106-111
97. Jentjens R, & Jeukendrup A. (2003). Determinants of post-exercise glycogen synthesis during short-term recovery. Sports Médicine (Auckland N.Z.). 33(2). 117-144.
98. McLellan TM, Pasiakos SM, Lieberman HR. (2014). Effect of protein in combination with carbohydrate supplements on acute or repeat endurance exercise performance : a systematic review. Sports Med. 44 :353-550.
99. Berardi JM, Price TB’ Noreen EE, et al. (2006). Postexercise muscle glycogen recovery enhanced with a carbohydrate-protein supplement. Med Sci Sport Exerc. 38 :1106-13.
100. Berardi JM, Noreen EE, Lemon PWR. (2008). Recovery from a cycling time trial is enhanced with carbohydrate protein supplementation vs isoenergetic carbohydrate supplementation. J Int Soc Sports Nutr. 5 :24.
101. Betts JA, Stevenson E, Williams C, et al. (2005). Recovery of endurance running capacity : effect of carbohydrate-protein mixtures. Int J Sport Nutr Exerc Metab. 15 :590-609.
102. Williams MB, Raven PR, Fogt DL, et al. (2003). Effects of recovery beverage on glycogen restoration and endurance exercise performance. J strength Cond Res. 17 :12-9.
103. Ivy JI, Res PT, Sprague RC, et al. (2003). Effect of a carbohydrate-protein supplement on endurance performance during exercise of varying intensity. Int J Sport Nutr exerc Metab. 13 :382-95.
104. Saunders MJ, Kane MD, Todd KM. (2004). Effects of a carbohydrate-protein beverage on cycling endurance and muscle damage. Med Sci Sports Exerc. 36 :1233-8
105. Saunders MJ, Luden ND, Herrick JE. (2007) Consumption of an oral carbohydrate-protein gel, improves cycling endurance and prevents post-exercise muscle damage. J Strength Cond Res. 21 :378-84.
106. Zawadzki KM, Yaspelkis BB, Ivy JL (1992) Carbohydrate-protein complex increases the rate of muscle glycogen storage after exercise. J Appl Physiol. 72,1854-1859.
107. Ivy JI, Goforth HW, Damon BM, et al. (2002). Early postexercise muscle glycogen recovery is enhanced with a carbohydrate-protein supplement. J Appl Physiol. 93 :1337-44.
108. van Hall G, Shirreffs AM, Calbert JAL (2000) Muscle glycogen resynthesis during recovery from cycle exercise : no effect of additional protein ingestion. J Appl Physiol. 88, 1631-1636
109. Carrithers JA, Williamson DL, Gallagher PM et al. (2000) Effects of postexercise carbohydrate-protein feeding on muscle glycogen restoration. J Appl Physiol. 88, 1976-1982
110. Romano-Ely BC, Todd MK, Saunders MJ et al. (2006). Effect of an isocaloric carbohydrate-protein-antioxydant drink on cycling performance. Med Sci Sports Exerc. 38 :1608-16.
111. Betts J, Williams C, Duffy K, et al. (2007). The influence of carbohydrate and protein ingestion during recovery from prolonged exercise on subsequent endurance performance. J Sports Sci. 25 :1449-60,
112. Millard-Stafford M, Warren GL, Thomas LM, et al. (2005). Recovery from run training : efficacy of carbohydrate-protein beverage ? Int J Sport Nutr Exerc Metab. 15 :610-24.
113. Rowlands DS, Thorp RM, Rossler K, et al. (2007). Effect of protein-rich feeding on recovery after intense exercise. Int J Sport Nutr Exerc Metab. 17 :521-43.
114. Rowlands DS, Rössler K, Thorp RM, et al. (2008). Effect of dietary protein content during recovery from high-intensity cycling on subsequent performance and markers of stress, inflammation, and muscle damage in well-trained men. Appl Physiol Nutr Metab. 33 :39-51.
115. Howarth, K.R., Moreau, N.A., Phillips, S.M., & Gibala, M.J. (2009). Coingestion of protein with carbohydrate during recovery from endurance exercise stimulates skeletal muscle protein synthesis in humans. Journal of Applied Physiology {Bethesda, Md.), 106(4), 1394-1402.
116. Rowlands DS, Wadsworth DP. (2011). Effect of high-protein feeding on performance and nitrogen balance in female cyclist. Med Sci Sport Exerc. 43 :44-53.
117. Beelen M, Cermak NM, van Loon LJ, (2015). Performance enhancement by carbohydrate intake during sport : effects of carbohydrate during and after high-intensity exercise. Ned Tijdschr Geneeskd. 159(0) :A7465.
118. Pritchett K, Bishop P, Pritchett R, et al. (2009) Acute effects of chocolate milk and a commercial recovery beverage on postexercise recovery indices and endurance cycling performance. Appl Physiol Nutr Metab. 34 :1017-22.
119. Karp JR, Johnson JD, Tecklenburg S, et al. (2006). Chocolate milk as a post-exercise recovery aid. Int J Sport Nutr Exerc Metab. 16 :78-91.
120. Thomas K, Morris P, Stevenson E. (2009). Improved endurance capacity following chocolate sport drinks. Appl Physiol Nutr Metab. 34 :78-82.
121. Ferguson-Stegall L, Mc Cleave EL, Ding Z, et al. (2011). Postexercise carbohydrate-protein supplementation improves subsequent exercise performance and intracellular signalling for protein synthesis. J Strength Cond Res. 25 :2110-1224.
122. Lunn WR, pasiakos SM, Colletto MR et al. (2012). Chocolate milk and endurance exercise recovery : protein balance, glycogen, and performance. Med Sci Sports Exerc. 44 :682-91.
123. Sahlin K, Broberg S, Katz A. (1989). Glucose formation in human skeletal muscle. Influence of glycogen content. Biochem J. 258 :911-913.
124. Ren JM, Gulve EA, Cartee GD et al. (1990). Influence of reduced glycogen level on glycogenolysis during short-term stimulation in man. Acta Physiol Scand. 139 :467-474.
125. Spriet LL, Berardinucci L, Marsh DR et al. (1990). Glycogen content has no effect on skeletal muscle glycogenolysis during short-term tetanic stimulation. J Appl Physiol. 68 :1883-1888.
126. Spencer MK & Katz A. (1991). Role of glycogen in control of glycolysis and IMP formation in human muscle during exercise. Am J Physiol. 260 :E859-E864.
127. Piehl-Aulin K, Söderlund K, Hultman E (2000) Muscle glycogen resynthesis rate in humans after supplementation of drinks containing carbohydrates with low and high molecular masses. Eur J Appl Physiol. 81, 346-351.
128. Rowlands DS, Swift M, Ros M et al. (2012). Composite versus single transportable carbohydrate solution enhances race and laboratory cycling performance. Appl Physiol Nutr Metab. 37 :425-36
129. Wallis GA, Wittekind A. (2013). Is there a specific role for sucrose in sports and exercise performance? Int J Sport Nutr Exerc Metab. 23(6):571-83
130. Moriarty KT, Mcintyre DG, Bingham K et al. (1994). Glycogen resynthesis in liver and muscle after exercise : measurement of rate of resynthesis by 13C magnetic resonance spectroscopy. Magma. 2 :429-432.
131. Casey A, Mann R, Banister et al. (2000). Effect of carbohydrate ingestion on glycogen resynthesis in human liver and skeletal muscle, measured by 13C MRS. Am J Physiol Endocrinol Metab. 278, E65-E75.
132. Bowtell JL, Gelly K, Jackman ML et al. (2000). Effect of different carbohydrate drinks on whole body carbohydrate storage after exhaustive exercise. J Appl Physiol. (1985). 88(5) :1529-1536.
133. Morifuji M, Kanda A, Koga J, et al. (2010) Post-exercise carbohydrate plus whey protein hydrolysates supplementation increases skeletal muscle glycogen level in rats. Amino Acids. 38, 1109-1115.
134. Sahi T (1994). Genetics and epidemiology of adult-type hypolactasia. Scand J Gastroenterol. 29 Suppl202:7-20.
135. Evidence Report/Technology Assessment Number 192. (2010). Lactose intolerance and health. AHRQ Publication No. 10-E004
136. Rienzo TD, D’Angelo G, D’Aversa F, et al. (2013). Lactose intolerance: from diagnosis to correct management. Eur Rev Med Pharmacol Sci. 17(Suppl2):18-25.
137. Ingram CJE, Mulcare CA, Itan Y, Thomas MG, Swallow DM. (2009). Lactose digestion and the evolutionary genetics of lactase persistance. Hum. Gen. 124, 579-591.
138. Itan Y, Jones BL, Ingram CJ, Swallow DM, Thomas MG. (2010). A worldwide correlation of lactase persistance phenotype and genotype. BMC Evol. Biol. 10, 36.
139. TishkoV SA, Reed FA, Ranciaro A, Voight BF, et al. (2007) Convergent adaptation of human lactase persistence in Africa and Europe. Nat Genet. 39:31– 40
140. Scrimshaw NS, Murray EB. (1988). The acceptability of milk and milk products in populations with high prevalence of lactose intolerance. Am J Clin Nutr. 48(Suppl):1079-1159
141. Rosado JL, Allen LH, Solomons NW. (1987). Milk consumption, symptoms response and lactose digestion in milk intolerance. Am J Clin Nutr. 45:1457-1460
142. Carraccio A, Montalto G, Cavera G, Notarbatolo A. (1998). Lactose intolerance and self-reported milk intolerance: Relationship with lactose maldigestion and nutrient intake. J Am Coll Nutr. 17:631- 636
143. Peuhkuri K, Teuri U, Vapaatalo H, Korpela R. (2000). Lactose intolerance – a confusing clinical diagnosis. Am J Clin Nutr. 71:600-602
144. Welsh JD, Hall WH. (1977) Gastric emptying of lactose and milk in subjects with lactose malabsorption. Dig Dis. 22:1060-1063.
145. Dehkordi N, Rao DR, Warred AP, Chawan CB. (1995). Lactose malabsorption as influenced by chocolate milk, skim milk, sucrose, whole milk, and lactic cultures. J Am Diet Assoc. 95:484-486.
146. Vesa TH, Marteau P, Briet FB, Flourie B, et al. (1997). Effects of milk viscosity on gastric emptying and lactose intolerance in lactose maldigesters. Am J Clin Nutr. 66:123-126.
147. Vesa TH, Marteau PR, Briet FB, Boutron-Ruault MC, Rambaud J-C. (1997). Raising milk energy content retards gastric emptying of lactose in lactose intolerant humans with little effect on lactose digestion. J Nutr. 127:2316-2320.
148. La Presse, 22 juillet 2008, par Stéphane Champagne d’Isabelle Charêt. http://www.lapresse.ca/vivre/200809/08/01-651558-la-face-cachee-du-lait-au-chocolat.php
149. Ludwing DS & Willet WC. (2013) Three daily serving of reduced-fat milk, an evidence-base recommendation ? JAMA Pediatr. 167(9) :788-789
150. Davis C. (Dep. of Nutr. Harvard School of public health). (2010). Comment on report of the Dietary guidelines advisory committee on the dietary guideline for américans,
151. L’épicerie. Épisode 5, 29 octobre 2014. http://ici.tou.tv/l-epicerie/S2014E05?lectureauto=1
152. Lagacé-Simard, Jacqueline. Ph.D. (2011). Comment j’ai vaincu la douleur et l’inflammation chronique par l’alimentation. Montréal, Québec : Fides
Tips for Optimal Leanness
#1: Take Control of What You Put In Your Mouth
When people let their emotions drive their eating, they end up feeling out of control and always hungry. Instead, try making informed choices about what and how you eat. By taking control of what you put in your mouth you avoid the pitfalls of emotional eating and can be empowered by your decisions.
#2: Get Fat Adapted
Most people don’t have the metabolic machinery to effectively burn body fat. Instead they run on carbs all day. The solution is to restrict carbohydrates in favor of protein and fat for your first two meals of the day (or at least for breakfast) in order to force the body to fat. Anaerobic exercise such as weight lifting or sprinting will also improve your body’s ability to burn fat.
#3: Eat The Most High-Quality Proteins—10 Grams of EAAs At Every Meal
High-quality protein includes fish, meat, poultry, eggs, and Greek yogurt. Planning meals around these foods blunts appetite and keeps you full, while also preserving lean mass during fat loss;. Protein also keeps blood sugar steady and and increases resting energy expenditure because protein is the most metabolically costly food for the body to digest.
#4: Ruthlessly Take Care of Your Gut Health
The microflora that live in your gut play a pivotal role in establishing your body composition, cholesterol profile, and long-term heart health. Support it by eating foods with fermented probiotics and lots of plant foods. Studies of groups that eat traditional diets have excellent gut health due to the high intake of root tubers, leafy vegetables, fruit, and nuts.
#5: Eat Fats That Are Good For You
Healthy fats are necessary for optimal hormone function and they provide bioavailable nutrients that will support a lean, muscular body composition. They are also delicious and filling. Good fats include those from olive and coconut oil, nuts, avocados, eggs, dairy, wild fish, and organic meat.
#6: Eat. Real. Food.
Most processed foods are engineered to trigger food intake and make you eat more calories. Processed foods also have a lower thermic effect than whole foods, meaning that if you eat a processed meat sandwich with white bread, your body will burn fewer calories during digestion than if you ate the same amount of calories from chicken breast, rice, and sweet potatoes.
#7: Favor Plants Over Grains.
Favoring vegetables instead of grains is an easy way to fill you up and increase nutritional density, but with fewer calories. Grain-based foods, whether it's good bread, crackers, rice, or cereal are very easy to overeat and they tend to crowd out other more nutritious foods.
#8: Save Higher Carb Foods For Dinner/Post-Workout
After working out your muscles are starving for nutrition. They are extra sensitive to insulin so that any carbs you eat will be stored as glycogen instead of fat. This makes post-workout the perfect time to enjoy higher carb foods. Further, including complex carbs at dinner will help lower cortisol and raise serotonin for restful sleep.
#9: Invest In Organic Meat, Eggs & Dairy
Organic meat, eggs, and dairy are significantly more nutritious than conventional versions and they help you avoid growth hormones and pesticides that may have estrogenic activity. High chemical estrogen intake is associated with higher body fat and worse health.
#10: Strength Train & Do Sprints—Proper Exercise Makes Everything Better
Don’t let lack of exercise be your blind spot. Exponentially greater benefits will come if you combine training and the optimal diet. Find a way to make it fun so that you enjoy movement—it’s what you were put on this earth to do!
The Agility Training Fallacy
This video explains why foot turnover speed is impressive but has no transfer of training to agility. Here it is explained in depth so as to put an end to pointless ladder drills that are not making you a better athlete. Video courtesy of Sport Science Collective
If you enjoyed the video check out this article: LADDER DRILLS DO NOT INCREASE SPORT PERFORMANCE UNLESS PERFORMANCE IS YOUR SPORT
Speed Notes
Speed is king for athletic performance, and the development of power is crucial. The athlete must “close the gap” between their maximal force output and their limit strength, and the faster they can achieve this, the more explosively they can perform. This can be achieved by utilizing Dr. Hatfield’s C.A.T. (Compensatory Acceleration Training) method. Essentially, this means completing reps explosively throughout the entire range of motion, so as leverages become more advantageous, the trainee continues to move the bar as fast and as hard as they can. A rep performed in this manner should not take more than ¾ of a second and one should use at least 60% of their 1RM, but not be so heavy as to slow down the rep speed.

The Core. What is it? And why should you care?
Core exercises are an important part of any strength training program, especially for those just starting out. Many people think that the occasional crunch will be enough to solve any issues they have when it comes to a lack of core strength, however this approached leaves many muscles of the core neglected. Let’s find out why…
What is the Core?
The core is often thought of as just the abs, which makes it understandable as to why sit-ups are seen as the go-to exercise. Unfortunately, it is not that simply. Think about the core as a muscular box where the abdominals make up the front, the paraspinals and gluteals sure up the back, the diaphragm as the roof, and the pelvic floor and hip girdle musculature as the floor.

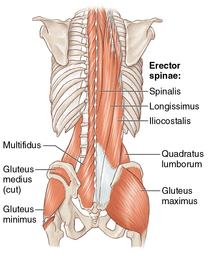


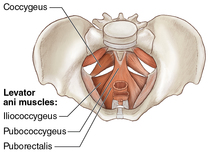
This intricate construction can be understood simply as the body’s foundation for movement. It is the central region providing a girdle of strength and connecting the abdomen with the lower back and hips. These muscles, together with the spinal muscles, create a stable base for generating strength and providing support for all movement.
Core Anatomy:
- Abdominals – the abdomen is a group consisting of four muscles: The rectus abdominis, also known as the “six-pack” is a superficial muscle sitting on the outermost layer of the core and is mainly involved in flexion. The transversus abdominis, which rests under the rectus abdominis, wraps around the core holding it together like a girdle and works to maintain good posture. Often times the in people with lower back pain the transversus abdominis is very weak. The internal obliques are deep muscles that help the body to rotate and flex to the side. The external obliques are another superficial musculature of the core just above the internal obliques which are important for rotational movements and side flexion.
- Paraspinals – made up of two major groups of lumbar extensors: the erector spinae and the “local” muscles (multifidus, rotatores, and intertransveri). The erector spinae is a group of three long tendinous muscles that run the entire length of the spine which provide support for spinal flexion (bending forward), extension (bending backwards) and aid in stabilizing the spine against lateral movement. The “local” muscles, mainly the multifidus is set deep and attached to the spine so that they may work to keep the spine straight and help stabilize through maintaining good posture.
- Hip Girdle & Gluteal Musculature – playing an important role within ambulatory activities such as stabilization of the trunk and pelvis and by transferring force from the legs to the pelvis and spine. The hip musculature consists of the psoas muscle group and the gluteus muscle group. The psoas, also referred to as the hip flexors, control flexion movements at the hip such as walking, running and climbing stairs. And for the gluteal musculature is made up of three muscles: the smallest being gluteus minimus, which lies beneath the gluteus medius, and works to lift the leg outward (abduction) as well as to internally rotate the hip. The gluteus medius sits just above the minimus, it assists with abduction, rotation (both internal and external) and provides stability to the pelvic region. The gluteus maximus is the largest of the three, it works to abduct and extend the hips in addition to stabilizing the pelvic region.
- Diaphragm & Pelvic Floor – The diaphragm serves as the roof of the core by providing stability to the lumbar spine via contraction during breathing. The pelvic floor musculature is coactivated with any transversus abdominis contraction and assists in stabilizing during movement.
- Quadratus Lumborum – A large, thin, quadrangular-shaped muscles that directly inserts into the lumbar spine. The quadratus lumborum works to stabilize the spine against lateral movement, lifting heavy objects and carrying items in one hand.
Why should we care about strengthening the core?
Strengthening the core musculature fights structural imbalances leading to such discomforts as low back pain which is one of the major forms of musculoskeletal degeneration in the adult population, affecting upwards of 80% of all adults. Research has shown that lower back pain is predominant among those who work at a desk, as sitting for long of time in a chair can cause the important muscles of the core to atrophy. Therefore, developing strength within this musculature is essential for maintaining a healthy posture, and leading a pain-free life.
What is an example of a core strengthening exercise?

Sliding Rollout from Knees
- Assume a kneeling position. Place both hands out in front of you on something that can move freely. An ab wheel, a Swiss ball, floor sliding discs or small hand towels will work. Think about squeezing all those muscles we just learned about and keep the head and neck in a neutral position.
- Lower your body under control by extending the hips and flexing the arms until your body approaches the floor. Keep the core and especially the gluteals contracted forcefully.
- Rise back to the starting position.
*The rollout is one of the best core strengthening exercises for beginners. If you use proper form and keep the core contracted, preventing the pelvis from rotating forward, your lower abdominals will receive even more of a workout. Break into this exercise gradually and make sure you keep the body in a straight line at the bottom of the movement. Many people sag at the hips or allow too much anterior pelvic tilt during the rollout exercise.
Just remember, core exercises should be seen as ones that not only help your “six-pack” but strengthen your lower back and pelvis. Having all these work together in harmony leads to better balance and stability, whether you’re on the field playing or completing daily activities.
What is Functional Strength Training?

Do you live to exercise? Unless you are an athlete, you probably answered no to that question. Most people are simply looking to improve their quality of life and would likely say that they exercise to live. And that is the focus of Functional Strength Training – to develop a foundation of strength and mobility within the body so that it may accomplish daily activities more easily.
What is Functional Strength Training?
Functional Strength Training exercises are designed to train and develop your muscles to make it easier and safer to perform everyday activities, such as carrying groceries, picking objects up off the ground, or playing a pick-up game of basketball. A typical workout will incorporate various movements using muscles from the upper and lower body, as well as everything in between.
What is an example of a Functional Strength Training movement?
Functional exercises tend to be multi-joint, multi-muscle movements.

A squat is a functional strength exercise because it trains the muscles used when you rise up and down from a chair or pick up low objects. You can see that it is both multi-joint and multi-muscle; incorporating the joints of the ankles, knees and hips, and the muscles such as the quadriceps and gluteal muscles. By training your muscles to work the way they do in everyday tasks, you prepare your body to perform well in a variety of tasks.
What are the benefits?
The benefits are multifaceted. Functional Strength Training, properly applied, will allow for a better quality of life by making everyday activities easier. With an increase in muscular strength, your body will become more functionally sound leading to improvements in balance, agility and help reduce the risk of falls.
Is Functional Strength Training for everyone?
Yes! Functional Strength Training is for everyone, as it can be adapted to any fitness level. If you are just starting out, you may only need to use your own body weight for resistance. As you become more fit and ready for more of a challenge, you can progress to using weights as your primary form of resistance.
What is the payoff?
As you add more functional strength exercises to your workout, you should see improvements in your ability to perform your everyday activities, and, thus in your quality of life. That is quite a return on your exercise investment.
For more information on how you can get started with a Functional Strength Training routine please contact: Stay Strong | Strength & Conditioning today!
For Fat Loss & Building Strength - Sprint Don't Walk!

#1: Burn More Belly Fat with Sprint Intervals
A large number of convincing studies show that high-intensity interval training is the best conditioning strategy for losing belly fat. In contrast, one research group that has conducted a number of experiments comparing aerobic and anaerobic training for belly fat loss write, “Disappointingly, aerobic exercise protocols have led to negligible fat loss.”
The reason anaerobic interval training works so much better is that it requires the body to adapt metabolically—your body is forced to burn fat to sustain the level of intensity being asked of it. It also elevates energy use for more than 24 hours post-workout, which has a dramatic effect on belly fat loss.
For example, a 2008 showed that a 6-week program increased the amount of fat burned during exercise by 12 percent and decreased the oxidation of carbohydrates—obviously, a favorable result for losing fat. More impressive, a 2007 study showed that in as little as 2 weeks, active women who performed interval training experienced a 36 percent increase in the use of fat for fuel during exercise.
Interval training is so effective for fat loss because it taps into different energy pathways than aerobic exercise. Simply, aerobic exercise tends to burn carbohydrates first and activate pathways that are degrading to muscle, whereas high-intensity exercise such as weight lifting and sprinting will burn a greater percentage of fat, enhance the body’s production of enzymes involved in fat breakdown, and activate pathways that lead to muscle development.
The other reason anaerobic intervals are superior for belly fat loss is that they increase excess post-exercise oxygen consumption (EPOC) a huge amount. A 2006 review showed that protocols that are more anaerobic in nature produce higher EPOC values than steady-state aerobic training because the trained muscle cells must rest restore physiological factors in the cells, which translates to a lot of energy expenditure.
Additional research on high-intensity training (HIT) programs noted that “the effect of regular aerobic exercise on body fat is negligible” whereas research into high-intensity exercise “indicates that it may be more effective at reducing subcutaneous and abdominal (visceral) body fat than other types of exercise.”
One study that compared the effect of high-intensity exercise (60 sprints of 8 seconds each, 12 seconds rest) with aerobic exercise (60 percent of maximal oxygen uptake for 40 minutes) found thatHIT resulted in significant decreases in overall fat mass, while the aerobic exercise group had a fat gain of 0.44 kg on average. The HIT group also had a significant 9.5 percent decrease in visceral fat, whereas the aerobic group had a non-significant increase of 0.2 kg or 10.5 percent. Of related interest is that the HIT group decreased fasting insulin significantly more than the aerobic group (31 versus 9 percent).
A second study found that in men with type 2 diabetes, an eight-week program that mixed aerobic and anaerobic exercise (twice a week of 45 minutes of aerobic exercise at 75 percent of max, and once a week of 5 sprints for 2 minutes at 85 percent) had a significant 44 percent decrease in visceral fat, with a 58 percent improvement in insulin sensitivity. They had no change in bodyweight but did have a 24 percent increase in thigh muscle cross sectional area, indicating muscle development, which accounted for the fact that they didn’t decrease bodyweight.
A third study performed on obese women compared a 16-week low-intensity protocol with a high-intensity protocol, based on rating of perceived exertion—not a very scientific indicator, but I’ll mention it anyway. The protocols produced comparable volumes of work as well as almost equal calories burned and miles completed. Despite this, only the HIT protocol yielded significant changes in metabolic markers or visceral fat loss. They lost significantly more total and visceral fat than the low-intensity group. Interestingly, both groups had similar exercise adherence to the program with 80 percent of each group completing the study, indicating that the high-intensity protocol was not too demanding for an obese, previously untrained population.
High-intensity exercise is effective because it increases exercise and post-exercise fat burning and may yield decreased post-exercise appetite. During exercise and after HIT, fat burning increases to remove built up lactate and hydrogen ions. Elevated growth hormone also supports fat burning and is a result of HIT programs.
#2: Lose Belly Fat With Sprint Intervals: The Proof
The following are examples of the superiority of anaerobic interval training for belly fat loss from the research:
- A 12-week high-intensity interval training program produced a 17 percent decrease in belly fat in overweight young men. Subjects lost 1.5 kg of belly fat and 2 kg of total fat, while building 1 kg of muscle. Fat burning was increased by 13 percent due to the 3-day a week program of 20-minutes of cycling in which the subjects sprinted for 8 seconds and then did 12 seconds of recovery, repeating these intervals for a total of 60 sprints.
- The same 20-minute cycling interval program produced 2.5 kg of fat loss in young women in 15 weeks, and the majority of the fat loss come from the legs and abdominal area. The sprint intervals were compared to a steady-state aerobic program that produced no fat loss.
- A 16-week study had trained athletes perform either a sprint interval protocol or steady-state running four days a week. The sprint interval protocol varied each day, but an example of one of the workouts used was 10 intervals of 30-sec sprints with 90 seconds rest. The sprint interval group lost 16 percent or 1 kg of visceral fat as well as 2 kg of total fat, compared to the endurance group that lost no belly fat, but did lose 1.4 kg of lean mass. The belly fat loss appears to be small, but be aware that subjects were lean, trained athletes to begin with and had less belly fat to lose than overweight subjects.
- An 8-week interval program using both high- and moderate-intensity intervals decreased belly fat by 44 percent in middle-aged men with type 2 diabetes. Subjects increased quad muscle size by 24 percent and improved insulin sensitivity by 58 percent—a dramatic improvement that highlights the other mechanisms involved in belly fat loss (muscle building, insulin health & blood sugar management).
#3: Sprints Take Less Time than Aerobic Exercise
Not only do sprints help you lose MORE belly fat, they help you lose it FASTER and with LESS training time. Repeatedly, studies show that more fat loss is achieved in high-intensity programs that use 20 to 25 minutes of training time than those that use 45 or 50 minutes of aerobic training time.
Scientists write that anaerobic intervals are overwhelmingly preferable to aerobics for producing belly fat loss, and that the estimated optimal dose of aerobic exercise necessary to lose belly fat appears to be 3,780 calories expended per week. This is an enormous volume of exercise that would require 1 hour of moderate intensity aerobic cycling 7 days a week to burn 550 calories a day so that you could lose even a pound a week!
In less than half the time you can get better results with anaerobic training. A 1994 study is indicative of this: Participants did either 20 weeks of aerobic training or 15 weeks of intervals (15 sprints for 30 seconds each) and lost nine times more body fat and 12 percent more visceral belly fat than the aerobic group.
What is so interesting about this study is that the energy cost of the aerobic program over the whole study period was 28,661 calories, whereas for intervals it was less than half, at 13,614 calories. In less time, the interval group lost much more weight—nine times more weight. How do researchers explain it?
Aside from greater fat oxidation and higher EPOC, hormone response plays a major role…
#4: Sprints Improve Hormone Response for More Belly Fat Loss
Sprint intervals and anaerobic exercise in general improve your entire endocrine system. Both training modes enhance the cells’ sensitivity to insulin, making anaerobic training a successful treatment for diabetes.
Perhaps most important, anaerobic exercise also elevates growth hormone (GH) —a powerful fat burning hormone that helps restore tissue and build muscle—much more than aerobic training. GH is released by the body in greater quantities in response to physical stress above the lactate threshold, which is the reason heavy, sprints are so effective.
Another hormone called adiponectin that is released from fat tissue during exercise also helps burn fat. Emerging scientific evidence shows that any time you perform forceful muscle contractions, adiponectin is released, and then your body produces a substance called PGC1 that is like a “master switch” that enhances muscle and metabolic functions, thereby burning belly fat. Naturally, anaerobic training is most effective for increasing adiponectin and PGC1 to burn fat since sprints and especially weight lifting require extremely forceful muscle contractions.
#5: Anaerobic Training Produces Less Cortisol For More Belly Fat Loss
Cortisol is the stress hormone that is elevated when you are under both physical and psychological stress. Research shows cortisol is chronically higher in endurance athletes—one study found that aerobic athletes had significantly higher evidence of cumulative cortisol secretion in their hair than controls.
In addition, cortisol is generally elevated more following aerobic training than anaerobic training. Part of this has to do with the fact that strength training and intervals do elevate cortisol, but they also elevate anabolic hormones such as GH and testosterone that counter the negative effects of cortisol.
If GH and testosterone are not elevated, cortisol overwhelms tissue, having a catabolic effect that leads to gradual muscle loss and fat gain. By doing aerobic training without strength training, you will lose muscle, lower your metabolic, rate, and gain fat. Worst of all, high cortisol causes chronic inflammation, which lead to belly fat gain over time—all-around bad news!
#6. The more aerobic volume, the more your brain ages. Therefore, senile dementia in Olympic athletes is proportionate to the annual volume of aerobic works.
#7. Slow long distance aerobic work is not a guarantee of cardiac health. Actually top cardiologist Dr. Bijan Pourat considers it “junk exercise”. He espouses resistance training for cardiac patient.
#8. Aerobic training can help you lose fat if you are just starting to exercise. Although it is not the most effective type of exercise for fat loss, aerobic-style cardio can work if you are new to exercise.
The Duke study used sedentary, out of shape, overweight people. The aerobic training they did was fairly intense (80 percent of max heart rate), so it's no surprise that they lost body fat. Being overweight and out of shape, and then exercising at that intensity for 40 minutes 3 times a week for 8 months can clearly lead to fat loss.
#9: In the long run, aerobic training is useless for fat loss. In a Duke study the aerobic group only lost an average of 1.6 kg of fat (not much!) and they didn't build any muscle, which is where we see the fault in the plan. By decreasing body weight, the aerobic group lowered metabolism, while improving aerobic conditioning.
They were “in shape” and thinner, but no stronger, and they had decreased their resting energy expenditure. In order to maintain that fat loss, they would need to eat less, change their macronutrient proportions, or exercise longer and more intensely.
For example, in the 2006 study of runners, only the runners who tripled their weekly mileage from 16 km/week to 64 km/week did not gain fat over the 9-year study. That's a huge increase that would naturally triple the amount of training time required to prevent fat gain.
#10: Doing smart anaerobic training, you can lose more fat quicker, while building muscle so that you raise your metabolism. For example, in a study of women that compared an anaerobic resistance training program with an aerobic protocol, the heavy load training group lost nearly 5 kg of body fat, gained about 3 kg of muscle, and had dramatic increases in strength. The women who did the high rep, aerobic-style lifting program had no change in body composition.
The benefit of building muscle is that your hard work lasts longer if you quit exercising: A study that tested what happens when subjects stopped exercising for 3 months after doing aerobic or resistance exercise found that a resistance training group maintained improvements in strength, muscle, and cardiovascular fitness longer than an endurance group.
The benefit of resistance training is even more pronounced for people who are in shape. In trained male athletes, a 6-week heavy load strength training program with multi-joint lifts (deadlift, squat, military press, chin-up, and bench press) allowed them to lose 1 percent body fat , while gaining 1.3 percent muscle mass for a dramatic improvement in body composition.
Compare that to the Duke study: The aerobic group also lost 1 percent body fat but gained no muscle, resulting in a less valuable body composition; the resistance group lost 0.65 percent body fat percent and gained 2 percent muscle; the concurrent group lost 2 percent body fat and gained 1.4 percent muscle mass.
The most favorable body composition was seen with the concurrent group, but it took double the time. When you consider the long-term effect of such a time-consuming, stressful program, it certainly is suboptimal.
The Facts About Strength Training and Managing Chronic & Age Related Conditions

If you have a chronic or age related conditions such as heart disease, arthritis, diabetes, depression, asthma, osteoporosis or back or joint, strength training can have positive benefits. However, it is always important to talk with your doctor before starting any exercise routine as they may have advice on what exercises are safe and any precautions you may need to take while exercising.
How can strength training improve my condition?
If you have a chronic or age related condition, regular exercise accompanied with strength training can help you manage symptoms and improve your health.
Being physically active can help you improve your heart health and endurance. Strength training can improve muscle strength and make it easier to accomplish daily activities, slow disease-related declines in muscle strength, and provide stability to joints. Mobility or flexibility exercises may help you to achieve a greater range of motion within your joints so they can function better.
For example:
- Heart disease: Regular exercise can help improve your heart health. Recent studies have shown that interval training is often tolerated well in people with heart disease and can produce significant benefits.
- Diabetes: Regular exercise can help insulin more effectively lower your blood sugar level. Physical activity also can help you control your weight and boost your energy. 2
- Asthma: Often, exercise can help control the frequency and severity of asthma attacks.
- Back Pain: Regular low-impact activities can increase strength and endurance in your back and improve muscle function. Abdominal and back muscle exercises (core-strengthening exercises) have been shown to reduce symptoms by strengthening the muscles around your spine. 3
- Arthritis: Exercise can reduce pain, help maintain muscle strength in affected joints and reduce joint stiffness. 4
- Depression: Regular exercise has been proven to be beneficial for symptoms of depression, resulting in a happier mood. 5
- Osteoporosis: Incorporating resistance training, such as lifting weights has been proven to build bone density and reduces the risk of falls by improving stability. 6
What exercises are safe?
Your doctor might recommend specific exercises to reduce pain or build strength. Depending on your condition, you might also need to avoid certain exercise altogether or during flare-ups. In some cases, you may need to consult a physical or occupational therapist before starting to exercise.
If you have low back pain, for example, your best bet is to start with low-impact activities such as walking or swimming. Strength exercises are more specific but could consist of back extensions or abdominal work.
If you have diabetes, for example, you can start with a basic body-weight strength training routine that includes chair squats, or farmer walks.
If you have osteoporosis, for example, the exercises that will be best for you all depend on if one area of the body is more affected than another. A hip issue is different than a back issue. Just remember resistance is the key to success — weighted exercises are always going to be better than resistance bands.
How often, how much and at what intensity can I safely exercise?
It should always be understood that before starting an exercise routine, it is important to consult your doctor about what is best for you. If your doctor clears you to start exercising here are a couple things to keep in mind.
- How often: Beginners, of good health, can generally tolerate more work than more advanced trainees. It is important to be active in some way every day. Walking can be done daily, while strength training should be kept to 2-3 workouts a week.
- How much: If you haven’t been active for a while, start slowly and build up gradually. Your body is the best barometer, rest when you are tired and workout when you’ve recovered. The more you engage in exercising the better you will feel.
- What about intensity: Start moderate, don’t overdo it!
Do I need to take special steps before getting started?
Depending on your condition, your doctor might recommend certain precautions before exercising.
If you have diabetes, for example, keep in might that physical activity lowers blood sugar. Check your blood sugar level before any activity. If you take insulin or diabetes medications that lower blood sugar, you might need to eat a snack before exercising to help prevent low blood sugar.
If you have arthritis, be sure to never skip a warm-up before you exercise. The heat the body generates from warming up can relax your joints and muscles and relieve any pain you might have before you begin.
What else do I need to know?
Starting a regular exercise routine isn’t as tough as it may seem.
To help you get started, consider seeking a professional, like the ones at Stay Strong | Strength & Conditioning.

Getting Started with Weight Training
You see your friends are going to the local gym and getting results from their hard work — improved physique and muscle tone. You’d like to start a program to replicate the results, but do not know if you have the time or where to start. It’s not as hard as you think!
What is Weight Training?
Weight training is a type of strength training that uses weights for resistance. Weight training provides a stress to the muscles that causes them to adapt and get stronger, similar to the way aerobic conditioning makes you more fit.
Weight training can be performed with free weights, such as barbell and dumbbells, or by using weight machines. You can also increase your strength through other types of resistance exercises, such as by using your body weight or resistance bands.
When it comes to Weight Training, how much is enough?
You do not have to be in the weightroom for 2 hours a day to see results. For most people, short weight training sessions a couple times a week are more practical than extended daily workouts. Chances are, if you are at the gym for more than an hour you are making friends and not working out!
You can see significant improvement in strength with just two or three 30 minute weight training sessions a week. This frequency also meets activity recommendations for healthy adults.
The Department of Health and Human Services recommends incorporating strength training exercises of all the major muscle groups into a fitness routine at least two times a week.
Weight Training is all about technique?
Weight training offers important health benefits when done properly. But it can lead to injuries, such as sprains, strains and fractures if it is not done correctly.
For best results, consider these basic weight training principles:
- Learn proper technique: If you are new to weight training, work with a trainer to learn correct form and technique. However, even advanced athletes can benefit from an occasional brush up on their form.
- Warm up: Cold muscles are more prone to injury than are warm muscles. Try a moderate aerobic activity such as riding on a stationary bike or elliptical for 5 minutes prior to engaging in a weight training routine. Other equally effective warm-ups consist of dynamic stretching or simply doing a few light weight sets of a giving exercise to get the body primed to use a heavier weight.
- Looking at repetitions: Theories on the best way to approach weight training abound, including countless repetitions and hours at the gym. But research shows that novice weight trainees can benefit from 2-3 sets of 12 repetitions.
- Use the proper weight: The proper weight to lift will be heavy enough to tire your muscles within those 10 repetitions. If you get to rep 12 and feel like you can do another 5 reps, the weight is too light! You should be exerting a high level of effort to get up that last rep.
- Start slowly: If you’re a beginner, you may find that you’re able to lift only a few pounds. That is okay, we all need to start somewhere. Once your muscles, tendons and ligaments get used to weight training exercises, you may be surprised at how quickly you progress. Once you can easily do 12 repetitions with a particular weight, you are ready to gradually increase the weight.
- Take time to rest: To give your muscles enough time to rest, take one full day between exercising each specific muscle group.
What are the rewards of weight training?
Lean muscle mass naturally decreases with age. If you don’t do anything to replace the muscle loss, it’ll be replaced with fat. But Stay Strong is here to help you reverse the trend, no matter your age.
As your muscle mass increases, you’ll be able to lift weight more easily and for longer periods of time. You’ll also help to maintain your bone density, better manage your weight, and improve your body’s metabolism. So don’t wait. Get started today!
Stay Strong | Strength & Conditioning
21690 Red Rum Drive Suite 117
Ashburn, Virginia 20147