
These articles explore the body, the mind, the environment, and the systems that shape human health. Each piece is written to make complex ideas easier to understand, whether the topic is training, nutrition, sleep, stress, digestion, symptoms, physiology, disease, or the way modern life affects how we feel and function.
Strength, Health, & the Art of Living Well
Difference Between Lactic Acid & Lactate
By Andrea Cespedes
You'll hear "lactic acid" and "lactate" used interchangeably by trainers, coaches and other sports experts. Colloquially, people assume you mean the same thing when you use either term, but they are technically different. Lactate is produced by your body in response to aerobic exercise and serves as a fuel for the muscles, delays fatigue and prevents injury. Lactic acid contains one additional proton and is not produced by the body at all during exercise.
One Proton
The technical difference between lactate and lactic acid is chemical. Lactate is lactic acid, missing one proton. To be an acid, a substance must be able to donate a hydrogen ion; when lactic acid donates its proton, it becomes its conjugate base, or lactate. When you're talking about body's lactate production and lactate or lactic acid threshold, the difference is largely a matter of semantics. But, the body produces and uses lactate -- not lactic acid.
What Is Lactate?
During hard exercise, from running a race to surfing the waves, your breathing rate increases to deliver more oxygen to the working muscles. Some exercises are so intense -- such as lifting a heavy dumbbell or swimming away from a shark -- that your body cannot use oxygen fast enough as a source to create fuel. For these quick, intense bursts of activity, your body needs to move into anaerobic mode -- during which the stored energy in your body is broken down into a compound called pyruvate.
When you don’t have enough oxygen to perform activity, your body turns pyruvate into lactate to fuel the muscles. Fit folk can utilize this form of energy production for one to three minutes.
High Levels of Lactate
As the muscles work at intense levels, they become more acidic, which interferes with firing. Lactate isn't the cause of this acidity; it's actually an antidote to this muscle failing. As your muscles lose power and energy, lactate swoops in to help counteract the depolarization of the cells. This is the familiar burn in the muscles you feel when you just can’t do another rep. Lactate production is a protective mechanism that prevents the body from hurting itself. When lactate production can't continue to the levels needed to prevent the complete failure of the muscles, you reach your threshold.
High levels of lactate -- or, as it is sometimes called, lactic acid -- were once blamed for delayed-onset muscle soreness. Lactic acid or lactate are not responsible for the soreness. Rather, researchers believe it is due to micro tears in the muscles that occur during strenuous exercise.
A Measure of Athletic Success
Lactate is essential to the exercising process. It helps bolster the mitochondria, energy powerhouses inside each of your muscle cells. Increase the number of mitochondria in your cells, and you'll improve your stamina and strength. High-intensity interval training in which you do short bouts of very strenuous exercise at or near your lactate threshold followed by recovery is especially effective in developing your lactate threshold. The better able you are to process lactate, the greater your ability to push high levels of performance.
About 75 percent of the lactate you produce during exercise is used as this moderating energy source; the other 25 percent leaks into the blood, which is how scientists test lactate levels during exercise. At one time, it was thought that high-level athletes produced less lactate; it's more likely that these athletes are better able to utilize the lactate they produce and leak less into the bloodstream, so their tests show lower amounts.
The Liver & Detoxification (Part 1)
By Graeme Bradshaw
Did you ever want to know about how to look after your liver?
This is part of a detailed series of articles explaining liver metabolism related to detoxification. You will learn how and what to do to maintain optimal liver health.
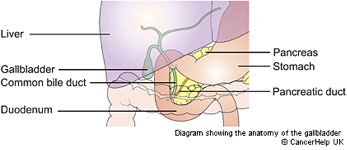
Where is the liver?
The Liver’s location is on the right side, at base of the ribs, shown in lilac color. The Gall Bladder sits under the liver.

Expanded view of the gall bladder ducts - the gall bladder is under the liver
The next diagram gives a better idea of the actual appearance of the liver, as well as how the blood flows into it from the intestines. It is the first place blood that having picked nutrients, like fats, amino acids, phyto-chemicals, vitamins and minerals and any wastes from the intestines and bowels. One of the liver's primary functions is filtering the blood. Almost 4 liters of blood pass through the liver every minute for detoxification. The blood then passes out to the heart.
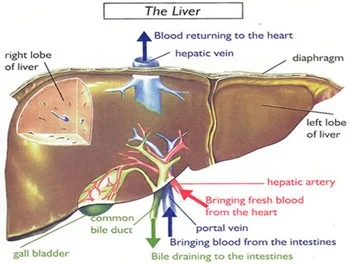
Bile from the liver is both a waste product, and it helps digesting and absorbing the fats and oils form food. Bile is especially released by fatty meals. Bile is necessary for bowel peristalsis, that is constipation may be caused by lack of bile.

Green colors above indicate the “biliary tree”, which are the bile ducts draining the liver into the gall bladder. These may be blocked with fatty cholesterol-laden plaque, bilirubin and bile salts, as depicted on the picture on the right side. The gall bladder may become congested with this plaque if it is not released as well and is prone to crystallize into gall stones by mid-life if the diet is incorrect. Read on for how to prevent this.
What are the functions of the liver?
- It is responsible for the production of bile that is stored in the gallbladder and released when required for the digestion of fats
- The liver stores glucose in the form of glycogen that is converted back to glucose again when needed for energy
- It also plays an important role in the metabolism of protein and fats.
- It stores the vitamins A, D, K, B12 and folate and synthesizes blood clotting factors.
- Another important role is as a detoxifier, breaking down or transforming substances like ammonia, metabolic waste, drugs, alcohol and chemicals, so that they can be excreted. These may also be referred to as "xenobiotic" chemicals.
Filtering the Blood
The liver plays a key role in most metabolic processes, especially detoxification. The liver is a filter designed to remove toxic matter such as dead cells, microorganisms, chemicals, drugs and particulate debris from the bloodstream. The liver filter is called the sinusoidal system, and contains specialized cells known as Kupffer cells that are part of the white blood cell immune function. They make up 10% of liver weight, and function to ingest and break down toxic matter.
Filtration of toxins is absolutely critical as the blood from the intestines contains high levels of bacterial waste, (endotoxins from the bowels), antigen-antibody complexes, and various toxic pollutants. When working properly, the liver clears 99% of the bacterial toxins during the first pass. However, when the liver is damaged, such as in alcoholics, the passage of toxins increases by over a factor of 10. This is similar if your intestines are too permeable, a condition known as “leaky gut”. Allergies (especially to gluten) and parasites may cause this.
The liver neutralizes a wide range of toxic chemicals, both those produced internally and those coming from the environment. The normal metabolic processes produce a wide range of chemicals and hormones for which the liver has evolved efficient neutralizing mechanisms. However, the level and type of internally produced toxins increases greatly when metabolic processes go awry, typically as a result of nutritional deficiencies, pesticide laden foods, low fiber diets and high red meat or alcohol intake.
Many of the toxic chemicals the liver must detoxify come from the environment: the content of the bowels and the food, water, and air. The polycyclic hydrocarbons (DDT, dioxin, 2,4,5-T, 2,3-D, PCB, and PCP), which are components of various herbicides and pesticides, are on example of chemicals that are now found in virtually all fatty tissues of the body, including the brain. Even those eating unprocessed organic foods need an effective detoxification system because all foods contain naturally occurring toxic constituents, and bacterial or fungal activity in the bowel may produce more.
So far we’ve learned that liver plays several roles in detoxification: it filters the blood to remove large toxins, synthesizes and secretes bile full of cholesterol and other fat-soluble toxins, and now we move on to how it enzymatically disassembles unwanted chemicals. This enzymatic process usually occurs in two steps referred to as phase I and phase II. Phase I either directly neutralizes a toxin, or modifies the toxic chemical to form activated intermediates that are then neutralized by one of more of the several phase II enzyme systems.
Proper functioning of the liver's detoxification systems is especially important for the prevention of cancer, since phase II detoxification deactivates carcinogens. Around 70% of all cancers are thought to be due to the effects of environmental carcinogens, such as those in pesticides, trans and burned fats in food, plastics and other sources of environmental estrogens, as well as air pollutants, cigarette smoke, etcetera. Our own hormones that are poorly detoxified may be cancer inducing, notably some forms of estrogens, and we are especially at risk if there is insufficient liver detoxification and bowel elimination. When combined with deficiencies of the nutrients the body needs for proper functioning of the detoxification and immune systems this issue gets worse. The level of exposure to environmental carcinogens varies widely, as does the efficiency of the detoxification enzymes, particularly phase II. High levels of exposure to carcinogens coupled with slow phase II detoxification enzymes significantly increases susceptibility to cancer.
Bile Excretion
The liver's second detoxification process involves the synthesis and secretion of bile. Each day the liver manufactures approximately 2 liters of bile, which serves as a carrier in which many toxic substances are dumped into the intestines. In the intestines, the bile and its toxic load are absorbed by fiber (if there is any in the diet) and then excreted. However, a diet low in fiber results in inadequate binding and reabsorption of the toxins back from the intestines into the liver. This low fiber diet (especially soluble fiber like oats and flax seed lignans) is a major cause of gall stones. This problem is magnified when bacteria in the intestine modify these toxins to more damaging forms.
The Gall Bladder : What does it do?
The gallbladder's main purpose is to concentrate and store your bile. Bile is a fluid made in the liver that helps you to digest fats in your small intestine. It is made from cholesterol, water, bilirubin and bile salts.
Bilirubin is what gives bile its greenish colour – the color turns darker brown the longer it is in the intestines. Bilirubin comes from the breakdown of used red blood cells.
When you eat fatty foods, the fats are broken down (digested) in your stomach and intestines. To get the bile to the food in your gut, your body either:
- Releases it from the liver and down the bile ducts, straight into your small intestine
- Stores it first in your gallbladder, which releases bile into your common bile duct as you need it
- Fats and oils in the diet stimulate the release of bile following a meal
- Fiber, especially soluble fibre such as from oats causes more bile to be released from the bowel, reducing gall stone formation. A low fiber diet increases gall stone risks, especially if no breakfast is eaten.
Factors causing most gallstone formation:
- A low fiber diet. Low fiber from too few vegetables, fruits, and whole-grain foods and whole grains such as oats or flax seeds. Do you eat 5 serves of fruit and vegetables a day or have a high fiber cereal breakfast? If not add oats and flax seeds which have high lignan content that is a soluble fiber.
- Too much red meat, cheese, and other dairy, bacon, sausages and gravies which are all high in saturated fat, that increase triglycerides (TG’s) and cholesterol, affecting the liver and gall (makes more concentrated bile).
- Omega 3 oil deficiency makes the TG’s and cholesterol go higher as well. Omega-3 oil, found in fish or flax seed oil, blocks cholesterol formation in bile.
- Sugar (and lack of exercise) increases triglyceride (TG’s) levels in the blood – high TG’s create less soluble bile. High sugar intake increases insulin levels that increase cholesterol saturation in bile (a bad effect).
- Irregular meals, skipping breakfast (“coffee breakfast”) and crash dieting contribute.
- Estrogens (the pill and oral contraceptives, and pregnancy increase frequency of gall stones – hence women more common sufferers). Women with a family history of gallstones are best to avoid oral contraceptive pills.
- Some gastrointestinal diseases – including Crohns disease.
- Some cholesterol lowering drugs (fibric acid derivatives e.g. Cliofibrate).
- Incidence of liver fluke is able to precipitate a particular type of pigmented gallstone and is relatively common in Asia (common especially if raw fish is regularly eaten).
- Food allergies are another trigger factor for gall related symptoms – if the gall is partly blocked consumption of food allergens trigger symptoms. The most common offenders are: egg, pork, onions/garlic, chicken, chocolate, dairy products chili, coffee, oranges, wheat, corn, beans and nuts in descending order. The high fat dairy products and pork are not recommended whether you have allergy/intolerance to them or not because of their saturated fat content.
- Coffee contracts the gall bladder – even if de-caffeinated – so if you have gallstones coffee may cause pain.
- Finally an odd one - sun-burning increases risk of gallstones.
Helpful Supplements and Nutritional Measures:
- Drink two large glasses of water on rising, and midmorning and mid afternoon to maintain the water content of the bile. Sliced un-peeled lemon in hot water is a bile stimulant too, and a healthy way to start the day. Add honey and some turmeric powder for anti-inflammatory benefits
- Take 2 fruits and 3 - 4 vegetable serves daily, especially including the cabbage family. This is for the fiber and important anti-oxidant content. (Carrots, beets, prunes, cabbage, broccoli, brussels sprouts, kiwi, papaya, apples are all very useful).
Lose excess weight (low animal fats and/or low sugar/sweets diet)
- Take extra mg vitamin C and 200 of vitamin E daily - improves bile solubility (Innate Response Antioxidant is our best antioxidant supplement)
- Fish oil ideally as 3 or 4 Krill Oil capsules daily (providing 750 - 1000mg of EPA and contains fat mobilizing phosphatidyl choline). We recommend this also for Fatty Liver. Oily fish include salmon, sardine, halibut herring, trout – twice or more weekly.
- Initially you need herbal bile stimulating herbs: Artichoke Extract is best and simplest for this, slightly lowering cholesterol and helping bowel movement along.
- Milk thistle can be used alternatively, having more benefits on detoxification and liver protection. A product giving Milk Thistle, Globe Artichoke and further nutrients as well (choline, methionine) called Liver Support – is often given for optimal liver-gall function.
- Exercising three times per week reduces gall stone formation.
- Take a probiotic - Lactobacilus bowel flora. These stimulate excretion of bile from the intestine, as well as binding these as well as other intestinal toxins and removing them.
Food Manufacturers Are Fooling You

Fact: The unhealthiest foods you could possibly eat often have the most health claims on the label. Ironic, isn't it? Think about most breakfast cereals. You're basically eating a bowl of sugar and flour. But the front of the box is packed with health claims:
- Low fat!
- Heart healthy!
- High fiber!
- Gluten-free!
- Reduced sodium!
- Made with whole grains!
Flip that box around like a smart grown-up and take a look at the ingredient list: sugar, flour, sugar in another form, sugar in a different color, sugar with a pretty name, etc. It's Type-2 diabetes in a bright box featuring a cartoon character selling love handles and loneliness.
And now they have a new marketing angle: a clever blend of childhood nostalgia and "fat acceptance." They tell us to eat what we want and love our body no matter what it looks like. Presumably, this is because they've finally recognized that the only people still eating cereal for breakfast have already given up on their health and body composition.
Funny thing is, when looking at the evidence, it's clear that there were never really health benefits in the first place to back up all these "healthy" labels. Here's how many of them originated and why they're wrong.
1 – Low Fat
It's taken over 40 years to officially call BS on the fraudulent claims about fat. The fear of dietary fat started in the 60's and 70's and immediately moved breakfast cereal into the "healthy" category. Hey, sugar is fat free! Bacon, eggs, and butter were out. Low-fat indigestible roughage was in because the research of the time was suggesting that saturated fat was clogging our arteries and increasing our risk of heart disease.
And despite the various top-notch review studies disproving this myth today, the cereal killers, sugar-water sellers, and big pharma phonies continue to lobby government officials, pay off medical and fitness professionals, and fund bogus research studies to keep it alive.
A low-fat diet isn't a benefit because eating fat doesn't cause disease. NOT eating it probably does, and we now know the body even needs some saturated fat to function optimally.
2 – High Fiber
Once you understand the origins of the low-fat guidelines it's easy to see how the advice to eat more fiber came about.
Denis Burkitt was the man behind the 1970's research linking high-fiber diets to lower rates of disease (colorectal cancer specifically). Just like Ancel Keys (the fat fraud), his evidence was awful. He basically claimed that African tribesman were healthier than Westerners because they ate their grains whole (with the fibrous outer shell). He conveniently failed to include a number of disease-free tribes thriving on starch-less diets high in saturated fat and animal protein, like the Masai.
Nonetheless, the bran we were throwing in the garbage became a prized possession, Burkitt wrote a best-selling book, and the "high-fiber" stamp fit perfectly next to the "low-fat" one on our breakfast bowl of blood sugar and body fat. It remains there today, right along with the misconception that whole grains are healthier than refined grains and that more fiber is a good thing, regardless of the source.
Meanwhile, the only study looking at the long-term impact of eating a high-fiber diet (DART, 1989) found an INCREASED risk of heart disease (23%) and mortality (27%). Those studies looking at colorectal cancer saw no benefit to upping our fiber intake:
"Our data do not support the existence of an important protective effect of dietary fiber against colorectal cancer or adenoma." (Fuchs CS et al. NEJM, 1999)
"In this large pooled analysis... high dietary fiber intake was not associated with a reduced risk of colorectal cancer." (Park Y et al. JAMA, 2005.)
3 – Cholesterol
The "lipid hypothesis" suggests that elevated cholesterol is associated with heart disease. And when we add it to what high-fiber, low-fat fanatics tell us, it's no wonder we think the way we do and fall for bogus health claims.
Right around the time all this low-fat, high-fiber evidence was surfacing, doctors and scientists were convinced they'd found the underlying cause of atherosclerosis – the narrowing and hardening of arteries. Nearly every doctor was on board with the theory. In the early 80's the National Institute of Health gathered 14 experts who voted unanimously that, "Lowering elevated blood cholesterol levels will reduce the risk of heart attacks caused by coronary heart disease."
They did so despite the fact that a causal relationship was never established, there's a library of evidence disproving it, and the original experiments used rabbits (herbivores that can't process dietary cholesterol) and a chemically prepared bare-cholesterol, which tends to oxidize.
But along came the prescription statins, and all of a sudden the questions and doctors aggressively opposing the theory disappeared. This created an environment where we dish out damaging side effects to more than 32 million Americans to lower the thing that's NOT associated with heart disease and does nothing to prevent it.
If cholesterol were associated with heart disease, there would be fewer heart attacks in those on statins and those with lower cholesterol, but there aren't. And there would be more heart attacks in those not on statins with higher cholesterol, but there aren't. The two variables aren't even related.
What we do see is statins causing mitochondrial and hormonal dysfunction, and lower cholesterol levels associated with cognitive and neurological impairment (Alzheimer's, Parkinson's, depression). This shouldn't come as a surprise when you understand that cholesterol is a building block for cell membranes, precursor to steroid hormones and essential nutrients, and fuel provider to neurons who can't generate it on their own.
"Our finding that low plasma cholesterol is associated with depressive symptoms in elderly men is compatible with observations that a very low total cholesterol may be related to suicide and violent death." (Morgan RE, et al. 1993, Lancet.)
Cereal fiber's ability to lower cholesterol is more of a detriment than a benefit. And realistically, the people getting heart attacks are the ones with elevated triglycerides, low HDL cholesterol, and excess small-dense (oxidizable) LDL particles – the same thing eating less saturated fat, more high-glycemic carbs, and vegetable oil-filled boxes of stuff claiming to "lower cholesterol" provides.
4 – Sodium
Heard the one about the obese, pre-diabetic guy with high triglycerides? Doc told him to eat less salt!
That's a joke. Or at least it should be. Salt doesn't make you fat and it's probably the last thing the average person needs to be worrying about when it comes to health.
High blood pressure is the fourth and final phase that turns Syndrome X into the Deadly Quartet. When you have metabolic syndrome, eating less salt won't do anything to solve the real problem.
- 2 weeks – insulin resistance (hyperinsulinemia)
- 2 months – elevated triglycerides (hyperlipidemia)
- 6 months – obesity (high bodyfat)
- 12 months – high blood pressure (hypertension)
People with high blood pressure don't need to eat less salt. They need to stop drinking liquid fructose and start driving-past instead of driving-thru.
More importantly, trying to abide by the FDA and AHA's recommendations to keep salt intake below 2400 mg per day (1tsp) increases cardiovascular disease risk and mortality from a heart attack or stroke. Ironically, this appears to be the result of elevated triglycerides and reductions in insulin sensitivity – the same thing driving the high blood pressure in the first place.
"The inverse association of sodium to CVD mortality seen here raises questions regarding the likelihood of a survival advantage accompanying a lower sodium diet." (Cohen HW, et al. AJM, 2006)
Therefore, one could say that your low-salt food is a double-whammy since you're consuming the food that's elevating the cause of high blood pressure and opting for the "lowers blood pressure" variety that's making it worse.
5 – Gluten
The gliadin proteins in wheat can be damaging to many people because of those proteins' ability to induce inflammation and increase intestinal permeability. Wheat itself may also cause cravings and interfere with your appetite-regulating mechanisms.
However, this doesn't mean all products with a "gluten-free" stamp of approval are suddenly health foods. Pizza is still pizza, pancakes are still pancakes, and a slab of pound cake beside your coffee is and always will be a bad choice... gluten-free or not. This should be common sense, but millions are willingly fooled every day because it's pretty easy to convince us that a delicious junk food is fine when it has an official-looking health claim on the box.
Just like we were tricked into selecting low-fat and low-sodium packaged products because of their apparent health benefit, food marketers have simply found another way to convince you that their bag or box of garbage is healthy.
Gluten-free cereal may be better than gluten-filled cereal, but it's still cereal. And you'd be better off leaving both for the birds.
References
- La Berg AF. 2008. How the Ideology of Low Fat Conquered America. J Hist Med Allied Sci 63(2):139-177.
- Siri-Tarino PW, et al. 2010. Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr 91(3):535-46.
- Skeaff CM and Miller J. 2009. Dietary fat and coronary heart disease: summary of evidence from prospective cohort and randomised controlled trials. Ann Nutr Metab 55(1-3):173-201.
- Yamagishi K, et al. 2010. Dietary intake of saturated fatty acids and mortality from cardiovascular disease in Japanese: the Japan Collaborative Cohort Study for Evaluation of Cancer Risk (JACC) Study. Am J Clin Nutr 92(4):759-65.
- Mente A, et al. 2009. A systematic review of the evidence supporting a causal link between dietary factors and coronary heart disease. Arch Intern Med 169(7):659-69.
- Limb M. 2014. Tougher action is needed to address "alarming" levels of overweight and obesity, says England's chief medical officer. BMJ 348:g2438.
- Burkitt DP. 1971. Epidemiology of cancer of the colon and rectum. Cancer 28(1):3-13.
- Mann GV, et al. 1971. Atherosclerosis in the Masai. Am J Epidemiol 95 (1): 26-37.
- Burr ML, et al. 1989. Diet and reinfarction trial (DART): design, recruitment, and compliance. Eur Heart J 10(6):558-67.
- Fuch CS, et al. 1999. Dietary fiber and the risk of colorectal cancer and adenoma in women. N Engl J Med 340(3):169-76.
- Park Y, et al. 2005. Dietary Fiber Intake and Risk of Colorectal Cancer: A Pooled Analysis of Prospective Cohort Studies. JAMA 294(22):2849-2857.
- Steinberg D. 2006. Thematic review series: the pathogenesis of atherosclerosis. An interpretive history of the cholesterol controversy, part V: the discovery of the statins and the end of the controversy. J Lipid Res 47(7):1339-51.
- Kellner A. 1952. Lipid Metabolism and Atherosclerosis: The Ludwig Kast Lecture. Bull N Y Acad Med 28(1):11-27.
- Stehbens WE. 2001. Coronary heart disease, hypercholesterolemia, and atherosclerosis. I. False premises. Exp Mol Pathol 70(2):103-19.
- Golomb BA and Evans MA. 2008. Statin adverse effects : a review of the literature and evidence for a mitochondrial mechanism. Am J Cardiovasc Drugs 8(6):373-418.
- Krumholz HM, et al. 1994. Lack of Association Between Cholesterol and Coronary Heart Disease Mortality and Morbidity and All-Cause Mortality in Persons Older Than 70 Years. JAMA 272(17):1335-1340.
- Braunwald E. 1997. Cardiovascular Medicine at the Turn of the Millennium: Triumphs, Concerns, and Opportunities. N Engl J Med 337:1360-1369.
- Prior IA. 1981. Cholesterol, coconuts, and diet on Polynesian atolls: a natural experiment: the Pukapuka and Tokelau island studies. Am J Clin Nutr 34(8):1552-61.
- Superko HR, et al. 2002. Small LDL and its clinical importance as a new CAD risk factor: a female case study. Prog Cardiovasc Nurs 17(4):167-73.
- Kendrick M. 2007. The Great Cholesterol Con: The Truth About What Really Causes Heart Disease and How to Avoid It. John Blake.
- Corona G, et al. 2010. The effect of statin therapy on testosterone levels in subjects consulting for erectile dysfunction. J Sex Med 7(4 Pt 1):1547-56.
- West R, et al. 2008. Better memory functioning associated with higher total and low-density lipoprotein cholesterol levels in very elderly subjects without the apolipoprotein e4 allele. Am J Geriatr Psychiatry 16(9):781-5.
- Huang X, et al. 2008. Low LDL cholesterol and increased risk of Parkinson's disease: prospective results from Honolulu-Asia Aging Study. Mov Disord 23(7):1013-8.
- de Lau LM, et al. 2006. Serum cholesterol levels and the risk of Parkinson's disease. Am J Epidemiol 164(10):998-1002.
- Shin JY, et al. 2008. Are cholesterol and depression inversely related? A meta-analysis of the association between two cardiac risk factors. Ann Behav Med 36(1):33-43.
- Perez-Rodriguez MM, et al. 2008. Low serum cholesterol may be associated with suicide attempt history. J Clin Psychiatry 69(12):1920-7.
- Seneff S. 2009. APOE-4: The Clue to Why Low Fat Diet and Statins may Cause Alzheimer's
- Morgan RE, et al. 1993. Plasma cholesterol and depressive symptoms in older men. Lancet 341(8837):75-9.
- Brown L, et al. 1999. Cholesterol-lowering effects of dietary fiber: a meta-analysis. Am J Clin Nutr 69(1):30-42.
- Swain JF, et al. 1990. Comparison of the Effects of Oat Bran and Low-Fiber Wheat on Serum Lipoprotein Levels and Blood Pressure. N Engl J Med 322:147-152.
- Barnard RJ, et al. 1998. Diet-induced insulin resistance precedes other aspects of the metabolic syndrome. J Appl Physiol 84(4):1311-1315.
- Alderman MH, et al. 1998. Dietary sodium intake and mortality: the National Health and Nutrition Examination Survey (NHANES I). 351(9105):781-785.
- Jurgens G and Graudal NA. 2003. Effects of low sodium diet versus high sodium diet on blood pressure, renin, aldosterone, catecholamines, cholesterols, and triglyceride. Cochrane Database Syst Rev 1:CD004022.
- Garg R. 2011. Low-salt diet increases insulin resistance in healthy subjects. Metabolism 60(7):965-968.
- Cohen HW, et al. 2006. Sodium Intake and Mortality in the NHANES II Follow-up Study. Am J Med 119(3):275e7-275e14.
- Fasano A, et al. 2003. Prevalence of celiac disease in at-risk and not-at-risk groups in the United States: a large multicenter study. Arch Intern Med 163(3):286-92.
- Troncone R and Jabri B. 2011. Coeliac disease and gluten sensitivity. J Intern Med 269(6):582-590.
- Fasano A. 2011. Zonulin and its regulation of intestinal barrier function: the biological door to inflammation, autoimmunity, and cancer. Physiol R 91(1):151-75.
- Fasano A. 2012. Zonulin, regulation of tight junctions, and autoimmune diseases. Ann N Y Acad Sci 1258(1):25-33.
Grains - The Real Cereal Killer
By Dr. Mercola
The persistent myth that dietary fat causes obesity and promotes heart disease has undoubtedly ruined the health of millions of people. It's difficult to know just how many people have succumbed to chronic poor health from following conventional low-fat, high-carb recommendations, but I'm sure the number is significant.
In the featured documentary, Cereal Killers, 41-year-old Donald O'Neill turns the American food pyramid upside-down—eliminating sugars and grains, and dramatically boosting his fat intake. In so doing, he improves his health to the point of reducing his hereditary risk factors for heart disease to nil.
Watching people's reactions to his diet brings home just how brainwashed we've all become when it comes to dietary fat. Most fear it. Yet they will consume sugar in amounts that virtually guarantee they'll suffer all the devastating health consequences they're trying to prevent by avoiding fat, and then some!
Fat versus Carbs—What Really Makes You Pack on the Pounds?
The fact is, you've been thoroughly misled when it comes to conventional dietary advice. Most dietary guidelines have been massively distorted, manipulated, and influenced by the very industries responsible for the obesity epidemic in the first place—the sugar and processed food industries.
Shunning the evidence, many doctors, nutritionists, and government health officials will still tell you to keep your saturated fat below 10 percent, while keeping the bulk of your diet, about 60 percent, as carbs.1 This is madness, as it's the converse of a diet that will lead to optimal health.
A recent Time Magazine2 article highlighted a report by the Environmental Working Group (EWG), which showed that many breakfast cereals contain more than 50 percent sugar by weight! Cereals marketed specifically to children are among the worst offenders. Kellogg's Honey Smacks and Mom's Best Cereals Honey-Ful Wheat topped the list with 56 percent sugar by weight. If you're looking for alternatives for your family you could try Snackimals from Barbara's. Snackimals is not on the EWG's list because it is a newer product. All of their flavors have only 7 grams of sugar per serving.
Even diabetes organizations promote carbohydrates as a major component of a healthy diet—even though grains break down to sugar in your body, and sugar promotes insulin resistance, which is the root cause of type 2 diabetes in the first place.
As noted in the film: "If we could get all diabetics to eat a high-fat, high-protein, low-carbohydrate diet, we would cut the insulin requirement so dramatically that it's been estimated that six pharmaceutical companies would go out of business tomorrow."Contrary to popular belief, you do not get fat from eating fat. You get fat from eating too much sugar and grains.
Refined carbohydrates promote chronic inflammation in your body, elevate low-density LDL cholesterol, and ultimately lead to insulin and leptin resistance. Insulin and leptin resistance, in turn, is at the heart of obesity and most chronic disease, including diabetes, heart disease, cancer, and Alzheimer's—all the top killers in the US.
Don't Fear the Fat
In the film, O'Neill switches over to a diet where 70 percent of his calories come from healthy fat—most of it in the form of macadamia nuts (my personal favorite)—and the remaining 30 percent of his caloric intake is divvied up between protein and fibrous fruits and vegetables. Over the course of 28 days, O'Neill:
- Loses weight and body fat
- Increases his lean muscle mass
- Feels more energetic and improves his athletic performance
- Increases his resting metabolic rate
- Improves his blood pressure, cholesterol, and other measurements to the point that he no longer has any risk factors for heart disease, which he's genetically predisposed for
Of particular importance here is that O'Neill's total cholesterol and LDL levels wentup, which initially caused significant concern. However, once they tested the LDL particle numbers, the results showed that his LDL particles were the largest species known, and he had virtually no small LDL particles at all.
This is phenomenal, as it's the small, dense LDL particles that cause inflammation. Large particles do not. Also, the markers for inflammation were virtually nonexistent, showing that he has no inflammation in his body at all. All in all, his one-month long high-fat, no-carb diet experiment proved that:
- Eating fat helps you lose fat
- Eating saturated fat decreases your risk factors for heart disease
- Regardless of your genetic predisposition your diet is, ultimately, the determining factor
I would also add that his results show the benefits of a high-fat, low-carb diet for athletes, many of whom are still convinced that this type of diet will make them heavy and sluggish. On the contrary, O'Neill breaks his own athletic record during his experiment, and refers to his renewed sense of vigor as feeling like a "spring lamb."
This high and sustained energy is a hallmark of ketogenesis, where your body is burning fat rather than sugar as its primary fuel. When your body burns fat, you don't experience the energy crashes associated with carbs.
Saturated Fat and Cholesterol Are Both Necessary for Optimal Health
Contrary to popular belief, saturated fats from animal and vegetable sources provide a number of important health benefits, and your body requires them for the proper function of your:

Cholesterol—another wrongly vilified dietary component—also carries out essential functions within your cell membranes, and is critical for proper brain function and production of steroid hormones, including your sex hormones. Vitamin D is also synthesized from a close relative of cholesterol: 7-dehydrocholesterol.
Your body is composed of trillions of cells that need to interact with one another. Cholesterol is one of the molecules that allow for these interactions to take place. For example, cholesterol is the precursor to bile acids, so without sufficient amounts of cholesterol, your digestive system can be adversely affected. It's also critical for synapse formation in your brain, i.e. the connections between your neurons, which allow you to think, learn new things, and form memories. In fact, there's reason to believe that low-fat diets and/or cholesterol-lowering drugs may cause or contribute to Alzheimer's disease.3
Replacing Refined Carbs with Healthy Fat—The Answer to Most of Your Health Concerns
Underlying most chronic diseases, including obesity, type 2 diabetes, heart disease, and cancer are inflammation and insulin/leptin resistance. When you eat carbohydrates, your blood sugar, insulin, and leptin will all temporarily rise, and these spikes are very pro-inflammatory. Where you have inflammation, disease and dysfunction follows. An excellent editorial in the journal Open Heart4 reviews the cardiometabolic consequences of replacing saturated fats with carbohydrates, which includes the following:

The answer, then, lies in avoiding these inflammatory spikes in blood sugar, insulin and leptin, and reversing insulin and leptin resistance. To do this, you need to:
- Avoid refined sugar, processed fructose, and grains. This means avoiding processed foods, as they are chockfull of these ingredients, along with other chemicals that can wreak metabolic havoc
- Eat a healthful diet of whole foods, ideally organic, and replace the grain carbs you cut out with:
- Moderate amounts of high-quality protein from organic, grass-fed or pastured animals (this is to ensure you're not getting the antibiotics, genetically engineered organisms, and altered nutritional fat profile associated with factory farmed animals)
- High amounts of high-quality healthful fat as you want (saturated and monounsaturated). Many health experts now believe that if you are insulin or leptin resistant, as 85 percent of the US population is, you likely need anywhere from 50 to 85 percent of your daily calories in the form of healthful fats for optimal health. Good sources include coconut and coconut oil, avocados, butter, nuts (particularly macadamia), and animal fats. Avoid all trans fats and processed vegetable oils (such as canola and soy oil). Also take a high-quality source of animal-based omega-3 fat, such as krill oil.
- As many vegetables as you can muster. Juicing your vegetables is a good way to boost your vegetable intake
Another "add-on" suggestion is to start intermittent fasting, which will radically improve your ability to burn fat as your primary fuel. This too will help restore optimal insulin and leptin signaling.
What's the Deal with Protein?
Dr. Rosedale, who was one of my primary mentors on the importance of insulin and leptin, was one of the first professionals to advocate both a low-carb and moderate protein (and therefore high-fat) diet. This was contrary to most low-carb advocates who were, and still are, very accepting of using protein as a replacement for the carbs.
The problem is that, along with grains, most Americans tend to eat far too much protein. While your body certainly has a protein requirement, there's evidence suggesting that eating more protein than your body needs could end up fueling cancer growth.
Dr. Rosedale advises limiting your protein to one gram of protein per kilogram of lean body mass (or 0.5 grams per pound of lean body weight). For most people, this means cutting protein down to about 35-75 grams per day. Pregnant women and those working out extensively need about 25 percent more. I believe this theory is worthy of consideration. The key though is to add healthy fat to replace the carb and protein calories you're cutting out of your diet. Again, sources of healthy fat include:

Your Health Is Within Your Control
Groundbreaking research by the likes of Dr. Robert Lustig and Dr. Richard Johnson (author of the books, The Sugar Fix and The Fat Switch) clearly identifies the root cause of obesity, diabetes, heart disease, and numerous other chronic diseases, and it's notfat. It's refined sugar—particularly fructose—consumed in excessive amounts. Their research, and that of others, provides us with a clear solution to our current predicament. In short, if you want to normalize your weight and protect your health, you need to address your insulin and leptin resistance, which is the result of eating a diet too high in sugars and grains.
For a comprehensive guide, see my free optimized nutrition plan. Generally speaking though, you'll want to focus your diet on whole, ideally organic, unprocessed or minimally processed foods. For the best nutrition and health benefits, you'll also want to eat a good portion of your food raw.
Sugar is highly addictive, and if you're like most people, you're no stranger to carb cravings. Just know that once your body gets used to burning fat instead of sugar as its primary fuel, those cravings will vanish. Many cereals and other grain products would not be quite as harmful if they didn't also contain so much added sugar. Even many organic brands contain excessive amounts. This is unfortunate, since many (Americans in particular) are really indoctrinated to eat cereal for breakfast. I've been working on a low-sugar cereal line for some time now, to provide a healthier alternative for those who really don't want to give up their breakfast cereal. I hope to have it ready sometime this summer.
Last but not least, for those of you still concerned about your cholesterol levels, know that 75 percent of your cholesterol is produced by your liver, which is influenced by your insulin levels. Therefore, if you optimize your insulin level, you will automatically optimize your cholesterol, thereby reducing your risk of both diabetes and heart disease.
Also, remember that even if a high-fat, low-carb diet was to raise your total cholesterol and LDL, it doesn't automatically mean that your diet is increasing your risk factors for heart disease. As O'Neill did in this film, you need to test your LDL particle number. Large-sized particles are good, while the smaller, denser particles can penetrate the lining of your arteries and stimulate the plaque formation associated with heart disease. The former does NOT increase your heart disease risk, while the latter one will. To learn more about LDL particle numbers and how to test them, please see my previous interview with Chris Kresser, L.Ac., which goes into this in some detail.
Too Much Protein??
Media sources often report, “too much protein stresses the kidney.” What does science say? Martin and colleagues reviewed the available evidence regarding the effects of protein intake on kidney function with a particular emphasis on kidney disease. The researchers found: “Although excessive protein intake remains a health concern in individuals with preexisting renal disease, the literature lacks significant research demonstrating a link between protein intake and the initiation or progression of renal disease in healthy individuals.” In addition “At present, there is not sufficient proof to warrant public health directives aimed at restricting dietary protein intake in healthy adults for the purpose of preserving renal function.” Protein restriction is common treatment for people with kidney problems.
Protein: The Facts, the Myths, and the Real Science
Everyone has an opinion about protein, and the myths surrounding it are rampant. That's why sorting the facts from the crap will lead to better choices regarding your own diet and protein intake. Answer the questions below and see if you've been falling for the myths.
Fact or Myth?
The RDA (Recommended Dietary Allowance) protein suggestions are just fine for people who work out.
Hint: The RDA guideline for protein is 0.8 grams per kilogram of bodyweight per day. So if you weigh 190 pounds (86 kilograms) you'd need about 69 grams of protein.
The Answer: Lifters and athletes concerned with their performance or physique require more protein than what's recommended by the RDA. So it's a myth (and a joke) that the RDA protein recommendations are adequate for ass-kicking individuals.
Here's Why: RDA protein recommendations are too low for certain groups. Those recommendations were never intended for people attempting to enhance performance, maintain, or gain muscle. In fact, a higher protein intake may have positive benefits regarding different health ailments including obesity, type 2 diabetes, osteoporosis, heart disease and muscle wasting.
The RDA guideline reflects the minimum daily needs of protein required to maintain short-term nitrogen balance in healthy, moderately active people. Nitrogen balance compares the amount of nitrogen coming into the body (from dietary protein) to the amount being lost. It's often used as a measurement of protein balance since protein is 16 percent nitrogen.
If you're consuming the same amount of nitrogen that you're losing, you're in nitrogen balance. If you're consuming more than you're losing, you're in positive nitrogen balance. If you're losing more than you're consuming, you're in negative nitrogen balance and are losing protein.
Nitrogen balance studies often involve examining urinary nitrogen levels. Approximately 90 percent of the nitrogen in urine is urea and ammonia salts – the end products of protein metabolism. The remaining nitrogen is accounted for by other nitrogen-containing compounds.
This nitrogen balance method is useful, but it has problems: Urine collections tend to underestimate nitrogen losses, dietary intake tends to be overestimated, miscellaneous skin and hair losses are prone to error, and the response to increased protein intake varies tremendously.
The Really Geeky Stuff
- In a review published in the International Journal of Sports Nutrition, researchers concluded, "Those involved in strength training might need to consume as much as 1.6 to 1.7 grams of protein per kilogram per day (approximately twice the current RDA) while those undergoing endurance training might need about 1.2 to 1.6 grams per kilogram per day (approximately 1.5 times the current RDA)."
- In another article published in Nutrition & Metabolism, researcher Donald Layman argued that the dietary guidelines should be improved and reflect new understandings about protein requirements. According to him, "During the past decade a growing body of research reveals that dietary protein intakes above the RDA are beneficial in maintaining muscle function and mobility." Diets with increased protein have been shown to improve adult health when it comes to treatment or prevention of obesity, type 2 diabetes, osteoporosis, heart disease and muscle wasting.
- A review published in the International Journal of Sport Nutrition and Exercise Metabolism was conducted to evaluate the effects of dietary protein on body composition in energy-restricted resistance-trained athletes, and to provide protein recommendations for these athletes.
The researchers concluded that "...the range of 2.3 to 3.1 grams per kilogram of FFM (fat free mass) is the most consistently protective intake against losses of lean tissue." In other words, for every kilogram on your body that's not fat, you should be consuming 2-3 grams of protein in order to preserve lean tissue. So if you have 190 pounds of lean tissue, up to 258 grams of protein would be optimal for you.
In addition, the goal of the athlete should be considered. Leaner athletes or those having a primary goal of maintaining maximal FFM should aim toward intakes approaching the higher end of this range. Even higher levels of protein than those recommended in the review are not uncommon in exercising individuals. It's unlikely that negative health consequences will follow from higher levels of intake, assuming there are no related health problems that would suggest limiting intake.
Fact or Myth?
The thermic effect of protein is the same as it is for carbs and fat.
Hint: The thermic effect of feeding or diet induced thermogenesis (DIT) is the amount of energy your body has to expend in order to digest and assimilate food. So picture a lean chicken breast (mostly protein), a bowl of rice (mostly carb), and tablespoon of butter (mostly fat). Which do you think your body will have to work hardest to digest?
The Answer: Among the three macronutrients, protein ranks highest in diet induced thermogenesis. So it's a myth that they're all equal in terms of their thermic effect. That means it'll cost you more calories to digest and absorb protein than it would fat and carbohydrate.
Here's Why: The consumption of protein requires an expenditure of 20-30% of the calories derived from protein. So, if 200 calories of protein are eaten, 40-60 calories are burned during digestion. DIT from carbohydrate is 15-20% and 2-5% for fat.
Fact or Myth?
Protein is more satiating (filling) than fat or carbohydrate.
Hints: Protein has an influence on CCK (cholecystokinin) and ghrelin. Protein may stimulate cholecystokinin (CCK) and decrease ghrelin. CCK is secreted mostly from the inner layer of the gastrointestinal tract has been shown to act as a satiety signal. The satiating effect of CCK was first demonstrated when administering CCK to rats. It "dose dependently" reduced meal size. Ghrelin is produced primarily in the stomach and has appetite increasing properties. Ghrelin levels are relatively high prior to a meal and they decrease after a meal.
The Answer: It's a fact that protein is usually more satiating than fat or carbs. When comparing protein, fat, and carbohydrate, protein is generally reported as the most satiating (satisfying to a point of full or beyond) and fat as the least satiating.
Here's Why: Research indicates that one of the primary factors involved with the satiating effects of protein is the thermic effect of feeding, mentioned above. Though protein's influence on ghrelin and CCK may play a large role in its satiating effects, more research needs to be conducted in these areas, as findings have been indecisive. Future research should concentrate on different levels of protein, different types of protein, and consumption of proteins in short and long term.
The Really Geeky Stuff
- A review published in Nutrition & Metabolism reported that protein induced thermogenesis has an important effect on satiety. "Protein plays a key role in body weight regulation through satiety related to diet-induced thermogenesis."
- A study published in Physiology & Behavior investigated the relative satiating effect of the macronutrients in lean women. On four separate occasions, the composition of an iso-caloric lunch "preload" was controlled in 12 lean women. Macronutrient composition had a significant effect on short-term hunger – the women were less hungry after the protein preload compared to the preloads with the other macronutrients. They also ate less after the protein preload.
- A study published in the American Journal of Clinical Nutrition tested the prediction that increasing protein while maintaining the carb content of a diet lowers body weight due to decreased appetite and decreased calorie intake. The study showed when increasing the protein intake from 15% of diet to 30% of diet (while eating the same amount of carbs) there was a decrease in appetite and fewer calories were consumed.
- The Journal of Clinical Endocrinology & Metabolism published a study that compared the effect of different proteins and carbohydrates on indicators of appetite and appetite regulatory hormones. CCK level was one of the primary outcomes measured.
Calorie intake was higher after the glucose preload compared with lactose and protein preloads. CCK level was higher 90 minutes after the protein preloads compared with glucose and lactose level. Researchers concluded that "acute appetite and energy intake are equally reduced after consumption of lactose, casein, or whey compared with glucose."
One Quick Caveat
The research sometimes gets a little messy. For example, some studies are indecisive when it comes to protein intake and ghrelin levels. This is why you need to rely on your own reasoning, logic, and experience while gathering info from the research.
References
- Blom, A.M., Lluch, A., Stafleu, A., Vinoy, S., Holst, J., Schaafsma, G., & Hendriks, H. (2006). Effect of high-protein breakfast ont he postprandial ghrelin response. The American Journal of Clinical Nutrition, 83(2), 211-220.
- Bowen, J., Noakes, M., Trenerry, C., & Clifton, P.M. (2006).Energy intake, Ghrelin, and Cholecystokinin after Different Carbohydrate and Protein Preloads in Overweight Men. The Journal of Clinical Endocrinology & Metabolism, 91(4).
- Helms, E., Zinn, C., Rowlands, D.S., & Brown, S.R. (2014). A Systematic Review of Dietary Protein During Caloric Restriction in Resistance Trained Lean Athletes: A Case for Higher Intakes. International Journal of Sport Nutrition and Exercise Metabolism, 24, 127-138.
- Layman, D.K.(2009). Dietary Guidelines should reflect new understandings about adult protein needs. Nutrition & Metabolism, 6(12), Lemon, P. (1998). Effects of exercise on dietary protein requirements. International Journal of Sports Nutrition, 8(4), 426-447.
- Lucas, M, & Heiss C.J.(2005) Protein needs of older adults engaged in resistance training: A review. Journal of Aging and Physical Activity, 13(2), 223-236.
- Moran, L.J., Luscombe-Marsh, N.D., Noakes, M., Wittert, G.A., Keogh, J.B., & Clifton, P.M. (2005). The Satiating Effect of Dietary Protein Is Unrelated to Postprandial Ghrelin. The Journal of Clinical Endocrinology & Metabolsim, 90(9).
- Poppitt, S.D., McCormack, D., & Buffenstein, R. (1998).Short-term effects of macronutrient preloads on appetite and energy intake in lean women. Physiology & Behavior, 64(3), 279-285.
- Weigle, D.S., Breen, P.A., Matthys, C.C., Callahan, H.S., Meeuws, K.E., Burden, V.R., & Purnell, J.Q. (2005). A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. The American Journal of Clinical Nutrition, 82(1), 41-48.
- Westerterp, K.R. (2004). Diet induced thermogenesis. Nutrition & Metabolism, 1, 1-5
What Enzymes Does Mercury Inhibit?
Mercury is a heavy metal that has been used for centuries as a medicine and a poison. Common exposures come from contaminated seafood, dental amalgams, and vaccines for infants. Mercury can exist in 11 different chemical states or compounds. At the molecular level, it forms bonds with sulfhydryl groups on an enzyme, which are parts of the enzyme that contain a sulfur atom that is attached to a hydrogen atom (SH). Binding of mercury can change the shape of the enzyme and block its activity. Enzymes inhibited by mercury include acetylcholinesterase, catalase, dipeptyl peptidase (CD26), amylase, lipase, lactase and glucose-6-phosphatase.
Acetylcholinesterase
Acetylcholine is one of the main neurotransmitters that nerves use to control muscle movement. After release, acetylcholine must be degraded in order to stop the “go” signal from continuing to stimulate the receiving cell. Acetylcholine is degraded by an enzyme called acetylcholinesterase. This enzyme is found in the synaptic cleft, which is the space between the "fingertips" of a nerve cell and the neighboring cell that the nerve activates. Mercury inhibits this enzyme differently in different species, depending on whether it can easily find a sulfhydryl group to latch onto. For human acetylcholinesterase, it takes millimolar amounts of mercuric chloride (HgCl2) to inhibit the enzyme.
Catalase
Catalase is an enzyme that converts hydrogen peroxide into water and oxygen. Hydrogen peroxide is regularly produced by cells as they make energy in a process called cellular respiration. Hydrogen peroxide is toxic at high levels, so cells get rid of it via the enzyme catalase. Though it is widely known that mercury inhibits catalase, it may do so by binding to sites other than sulfhydryl groups. It is interesting to note that when a person absorbs elemental mercury, which causes brain damage, catalase is the enzyme in the red blood cells that converts elemental mercury into an ionic form (mercuric salt).
Creatine Kinase
Mercury also inhibits the enzyme found in skeletal muscle called creatine kinase. Muscle cells contract by using an energy molecule called adenosine triphosphate (ATP), a molecule with three -- thus the “tri” prefix -- phosphates. Energy is released for an enzyme when the enzyme grabs ATP and breaks off one phosphate, resulting in adenosine diphosphate (ADP) -- “di” means two. A quick way of making ATP is to take a phosphate from a sugar molecule called phosphocreatine and add it to ADP. Creatine kinase is the enzyme that recharges ADP into ATP in this way. Mercury inhibits creatine kinase in several ways. Mercury blocks creatine kinase’s ability to bind ADP or the magnesium ion that the enzyme needs in order to function properly.
Digestive Enzymes
Mercury binds to sulfhydryl groups, which is found on the amino acid cysteine. Since cysteine is a common amino acid in many enzymes, mercury inhibits a whole host of enzymes. The "Journal of Applied Toxicology" reported the effects of inorganic mercury in the liver tissue of freshwater fish. Mercury inhibited many enzymes involved in digestion of food molecules, such as protein, carbohydrate and fat: amylase, lipase, lactase and maltase. Mercury also inhibited glucose-6-phosphatase, an enzyme involved in the production and export of glucose in cells.
A Heads-Up Look at Brain Health
Medical advances of today and the very near future — gene therapies, nanotechnology, targeted monoclonal antibodies, cloning, and more — will allow us to “repair” or “replace” damaged and diseased body parts and raise the average life expectancy to 100 years or more. The problem with this magnificent advancement is the studies which suggest that 40% of those reaching 85, and nearly 100% of those reaching 120, will be senile. Of what use is living to a ripe old age if we cannot enjoy it, or even be aware that we’re alive?
Brain Studies
Some 2000 years ago the ancient Greeks attributed all behavior to four temperaments: Hot, Dry, Moist, and Cold. The Romans attributed all symptoms and behaviors to four body fluids, which they called humors: Phlegm, Yellow Bile, Black Bile, and Blood. While Hippocrates, Galen, and hundreds of others slowly advanced the understanding of human anatomy and physiology, the brain sat unstudied for over 1500 years. It was not until the 18th and 19th centuries that brain anatomical science progressed to the point that four distinct lobes were identified, with specific behaviors and body functions ascribed to each.
Over the next 100 years, biochemical and pharmaceutical researchers discovered four separate brain chemicals, called neurotransmitters, that were used by the brain. Somewhat later, four distinct brain waves, or patterns of electrical activity, were discovered and correlated with specific lobes in the brain. Only fairly recently have researchers started to understand this most mysterious organ.
From the 1950s to present, psychiatrists and phychologists have described four broad classifications of human behavior: extroverted or introverted, intuitive or sensing, thinking or feeling, and perceiving or judging. If you suspect that these four primary behaviors can be assigned to a specific lobe, you’d be right!
Brain malfunctions, as manifested by psychiatric problems or unacceptable behavior, can be largely attributed to an imbalance of neurotransmitters within the brain. Unfortunately, discovering these levels within a living brain was not an easy task. (If you think a spinal tap is a risky procedure, just imagine a “brain tap” gone wrong!) What was needed was a simple, noninvasive test to measure the levels of neurotransmitters in a functioning human brain. Various scans of the brain can be employed, but they cannot show actual brain function. For example, an MRI of a patient’s brain right before death and right after death would be identical.
After 25 years of painstaking work, neurological researchers have finally uncovered a long-hidden piece of the puzzle — the relationship between the brain’s chemicals and the brain’s electricity. This discovery allowed clinicians to diagnose brain dysfunction with a simple, noninvasive assessment of the brain’s electrical activity. By measuring the four electrical components of brain activity, doctors can determine the levels of the four neurotransmitters and initiate treatment protocols to correct a deficiency of one or more of them.
Correlation Times Four
Four temperaments; four humors; four neurotransmitters; four lobes; four classes of human behavior; four brain waves; four electrical measurements of brain function. How do these relate? The following table shows the relationship between brain lobes, neurotransmitters, behaviors or personality types, and electrical measurements.

The table above shows the electrical measurements used to determine neurotransmitter levels. As a person ages, his brain goes through a slow decline, or “electropause,” in which the voltage, speed, rhythm, and synchrony change. By measuring these four electrical characteristics, a person’s “brain age” can be determined, which may be younger or older than typical for his chronological age. More importantly, a deficiency in one or more neurotransmitters can be detected and steps taken to restore normal levels.
A computerized diagnostic device called a Brain Electrical Activity Map (BEAM) measures these four values and creates a “picture” of the brain’s electrical activity. It records and tracks the progression of the positive wave created in the brain by an external stimulus, such as a sound (auditory evoked potential) or a flash of light (visual evoked potential).
Speed. A “normal” brain takes about 300 msec (milliseconds) plus a person’s age in years to “think.” This is the measurement of the time delay, or latency, between a stimulus given and the recognition of that stimulus in the brain. As the latency increases (speed decreases), a person moves from mild cognition deficits to severe dementia.
Voltage. A “normal” brain creates an electrical potential of about 10 µv (microvolts). The voltage generated in a person’s brain is related to his ability to concentrate, and low voltage can result in memory impairment, obesity, addictions, or schizophrenia.
Rhythm refers to the regularity of a person’s brain waves. Like cardiac rhythm, the more smooth the rhythm, the better. Brain-wave arrhythmias yield a spectrum of disorders from anxiety and recurring headaches to manic depression and seizures.
Synchrony is a comparison of the electrical activity in each of the hemispheres of the brain. It is common for a person to be dominant in one hemisphere or the other, but a severe imbalance in the electrical activity of the right vs. left hemisphere can lead to sleep disorders, IBS, somatization disorders, or phobias.
Acetylcholine
Review: A “normal” brain takes about 300 msec (milliseconds) plus a person’s age in years to “think.” This is the measurement of the time delay, or latency, between a stimulus given and the recognition of that stimulus in the brain. As the latency increases (speed decreases), a person moves from mild cognition deficits to severe dementia.
Acetylcholine-associated disease states
A diagnostic evaluation of a person’s brain speed can give objective evidence of disturbances in cognition, memory, attention, and behavior. After subtracting the patient’s age, the baseline latency measurement indicates the following: 300 msec is “normal”; 350 msec indicates mild to moderate disturbances in cognitive function (“muddled thinking”); 360 to 370 msec indicates ADD or variability of attention, errors of omission or commission, and delayed reaction time; 380 msec is typically found in Parkinson patients; 420 msec is the threshold for Alzheimer disease, with increasing latency as the dementia progresses. Early detection of deficiencies in the speed at which the brain operates can allow early intervention to slow or reverse the decline, possibly delaying or preventing the onset of Alzheimer and other dementias.
Beyond detecting a frank disease state associated with severe acetylcholine deficiency, physicians can analyze thebalance of the four neurotransmitters to determine a patient’s personality type.
The acetylcholine-dominant personality
Acetylcholine is produced in the parietal lobes, which are responsible for thinking functions such as language processing, intelligence, and attention. People with an excess of acetylcholine (about 17% of the world’s population) are adept at working with their senses and view the world in sensory terms. They are quick thinkers, highly creative, and open to new ideas. Flexibility, creativity, and impulsivity open them up to trying almost anything, as long as it offers the promise of excitement and something new; they are not afraid of failure. They love to travel and have a quest for lifelong learning. These people also tend to be extremely sociable, even charismatic. They love making new friends and put a lot of energy into all of their relationships, whether at work, at home, or in the community. They are eternally optimistic, romantic with their significant other, and attentive to the needs of their children. They are quite popular with a broad range of people. People with extremely high levels of acetylcholine, however, risk giving too much of themselves to others, even to the point of being masochistic. They may feel that the world is taking advantage of them, or they may become paranoid. Too much acetylcholine can drive a person into isolation.
The acetylcholine-deficient personality
Low levels of acetylcholine result when either the brain burns too much or produces too little. Shifts in personality occur at a much milder deficiency than the dementia- producing deficiencies mentioned earlier. These personality traits can, in fact, manifest when the acetylcholine level is only slightly lower than the levels of the other three neurotransmitters. And remember, we’re looking at the relative balance of neurotransmitters. A deficiency in one neurotransmitter is usually offset by an excess of another, which typically produces the personality traits associated with a dominance of that other neurotransmitter.
The eccentric. The absence of thought connections to other people and the world makes this person’s behavior seem odd. The eccentric usually steers away from human interaction and keeps himself isolated. Outwardly, he appears bland and inexpressive. When even mildly stressed, however, he can become a danger to himself and others.
The perfectionist. This person is usually hard working, detail oriented, devoted, and exacting. Self-discipline is a hallmark of this personality type, which can be either a plus or a minus, depending on the severity of the imbalance and which other neurotransmitter is dominant. This person can be an excellent worker, or he can be rigid and obsessive to the point that nothing is actually accomplished. The perfectionist’s life is usually lacking in enjoyment, relaxation, and warmth, which can make that person unapproachable.
Dopamine
Review: A “normal” brain creates an electrical potential of about 10 µv (microvolts). The voltage generated in a person’s brain is related to his ability to concentrate, and low voltage can result in memory impairment, obesity, addictions, or schizophrenia.
Dopamine-associated disease states
A person’s ability to concentrate can be directly correlated with his dopamine level. A diagnostic evaluation of the voltage in a person’s brain can give objective evidence of disturbances in concentration and memory. Low dopamine levels can be involved in difficulty performing routine tasks, a variety of sexual disorders such as loss of libido or anorgasmy, various addictions, from caffeine to opiates, and decreased physical activity due to fatigue. Obesity is a common result of the combination of sugar cravings and low physical activity associated with suboptimal dopamine levels in the brain.
Brain voltage can vary within the range of 0 µv (dead) to 20 µv (super concentration), with 10 µv being classified as “normal.” The voltage range correlates as follows: 0-2 µv is typically found in cocaine babies; 2-4 µv can indicate severe addictions, severe attention deficit disorder, or schizophrenia; 5-6 µv indicates a chronic brain disorder; 7 µv is found in those with moderate addictive behavior, such as caffeine and sugar cravings; 8-9 µv is typical for mild to moderate memory and thinking disturbances, including mild attention deficit; 10 µv is “normal”; and above 10 µv indicates an increased ability to concentrate, even to the rejection of external stimuli at the high end of the range.
Drugs that increase dopamine levels have been used as adjunctive therapy for schizophrenia and opiate addiction. Beyond detecting and treating frank disease states associated with a severe dopamine deficiency, physicians can analyze the balance of the four neurotransmitters to determine a patient’s personality type.
The dopamine-dominant personality
Dopamine is the source of the brain’s power and energy. People with an excess of dopamine (about 17% of the world’s population) thrive on energy. They are likely to be strong-willed individuals who know what they want and how to get it. They are highly rational, more comfortable with facts and figures than feelings and emotions. They can be self-critical, but do not accept criticism or negative feedback from others. These people function well under stress, focusing intently on the task at hand. They are tireless and typically need less sleep than average. Strategeic thinking, invention, and problem-solving are the hallmarks of these individuals. In their personal lives, they like activities related to knowledge and intellect. They can be competitive in sports, but prefer individualized sports over group sports. They tend to establish personal relationships easily, but may have trouble nurturing them. As highly rational people, they have trouble understanding that many people believe feelings are more important than reason. They have a tendency to want to exert control over their spouse and children, and a successful marriage depends on the loyalty and goodwill of the spouse.
People with extremely high levels of dopamine, however, can be overly intense, driven, and impulsive. They may turn to violence as a way of creating controlled environments of excitement and power. Teens may be driven to shoplifting, street racing, or date rape. Criminals — especially repeat sexual offenders — often have extreme dopamine levels and a heightened libido that frequently accompanies it.
The dopamine-deficient personality
Low levels of dopamine result when either the brain burns too much or produces too little. Shifts in personality occur at a much milder deficiency than the disease- producing deficiencies mentioned earlier. Personality shifts can, in fact, manifest when the dopamine level is only slightly lower than the levels of the other three neurotransmitters. And remember, we’re looking at the relative balance of neurotransmitters. A deficiency in one is usually offset by an excess of another, which typically produces the personality traits associated with a dominance of that other neurotransmitter.
Dopamine production determines the brain’s power, as measured by voltage. As the voltage becomes suboptimal, the person literally slows down, mentally and physically. Minor deficiencies can produce a range of mental and physical symptoms, such as mild memory loss, mild depression (“the blues”), panic disorder, PMS, insomnia, fatigue, mild hypertension, nicotine addiction, and obesity. Sexual side effects, such as loss of libido and difficulty achieving orgasm, are common among people with a dopamine deficiency.
The previous two neurotransmitters — acetylcholine and dopamine — can be thought of as the brain’s “on” switch, providing energy, power, and speed. The next two — gamma-aminobutyric acid (GABA) and serotonin — function as the brain’s “off” switch, providing calmness, rest, and sleep. A balance of the “on” and “off” neurotransmitters is necessary for proper brain function.
GABA
Review: Rhythm refers to the regularity of a person’s brain waves. Like cardiac rhythm, the more smooth the rhythm, the better. Brain-wave arrhythmias, or dysrhythmias, yield a spectrum of disorders from anxiety and recurring headaches to manic depression and seizures.
GABA-associated disease states
Gamma-aminobutyric acid (GABA) is the major inhibitory neurotransmitter in the brain. It has a calming, stabilizing effect. It controls the brain’s rhythm, which allows a person to function at a steady pace and prevent him from becoming too “hyper.” As the brain’s GABA level declines, brain waves begin to become less rhythmic. This can bring on a multitude of symptoms, both psychological and physical.
Mild brain-wave dysrhythmias can produce anxiety and its accompanying physical manifestations: restlessness, sweating, cold or clammy hands, butterflies in the stomach, and a lump in the throat. Other physical symptoms that can appear with a moderate GABA deficiency include carbohydrate cravings, an abnormal sense of smell, and unusual allergies. As GABA levels further decrease, anxiety can become more pronounced and produce attention-deficit disorders, PMS, flushing, trembling, hypertension, cystitis, and gastrointestinal disorders. At the most extreme deficiency, this can become full-blown panic attacks, manic depression, migraine headaches, hyperventilation, palpitations, tachycardia, blurred vision, tinnitus, twitching, and seizures. Advanced psychological symptoms can include severe delusions, feelings of dread, and a short temper that can progress into full-blown rage reactions and violence. Chronic marijuana and alcohol abuse can signal an acute GABA deficiency.
Beyond detecting and treating frank disease states associated with GABA deficiencies, physicians can analyze thebalance of the four neurotransmitters to determine a patient’s personality type.
The GABA-dominant personality
People with high GABA levels (about 50% of the world’s population) share the common attributes of stability, consistency, sociability, and concern for others. They are nature’s most dependable people. They can be counted on to show up at work every day and be there when others need them. At work, GABA- dominant people are the ones who set goals, organize projects, schedule activities, and keep others on task. Their punctuality, objectivity, practicality, and confidence make them excellent employees. Organization is paramount to them — at work, at home, and in their social life. It’s no wonder that these people gravitate to careers as administrators, accountants, air-traffic controllers, meeting planners, nurses, EMTs, and yes, medical transcriptionists. They’re the ones in the group who stay focused on the matter at hand. They are the consummate team player, both metaphorically and literally. In their personal life, such people derive pleasure from taking care of their family and friends. They can be a serene island in a sea of chaos. Although they like group activities, they cherish one- on- one relationships. Their friends are forever, and their marriage is a long- term commitment. Nurturing and making others happy is their ultimate goal. They tend to be religious and believe in traditions, especially where friends and family are involved, such as holiday gatherings.
As with the other neurotransmitters, it is possible to have too much of a good thing. People who produce too much GABA can be organizational to the point of setting rigid schedules and micromanaging others, whether as a boss, a coworker, a friend, or spouse. Excess GABA can dramatically increase a person’s nurturing tendencies. They can spend enormous amounts of time and energy looking for opportunities to give love and care to others, at the cost of their own needs not being met.
The GABA-deficient personality
Low levels of GABA result when either the brain burns too much or produces too little. Shifts in personality occur at a much milder deficiency than the disease- producing deficiencies mentioned earlier. Personality shifts can, in fact, manifest when the GABA level is only slightly lower than the levels of the other three neurotransmitters. And remember, we’re looking at the relative balance of neurotransmitters. A deficiency in one is usually offset by an excess of another, which typically produces the personality traits associated with a dominance of that other neurotransmitter.
Unlike a balanced brain that creates energy in a smooth, steady flow, a person with low GABA creates energy in bursts. This brain dysrhythmia can upset the body in a number of ways, but none is more pronounced than in the realm of emotional well- being. Specifically, he can lose the ability to effectively deal with life’s stresses. He may begin to feel nervous, anxious, and irritable. He may demonstrate poor emotional stability, lack impulse control, and resort to childish behavior. It can also manifest as poor verbal memory and difficulty concentrating. Physically, low GABA levels can bring on a variety of subacute conditions such as allergies, transient aches, instability while walking, diarrhea or constipation, and insomnia or hypersomnia. Usually, such physical annoyances occur one after another to the point that a person begins to wonder about his general state of health.
Serotonin
Review: Synchrony is a comparison of the electrical activity in each of the hemispheres of the brain. It is common for a person to be dominant in one hemisphere or the other, but a severe imbalance in the electrical activity of the right vs. left hemisphere can lead to sleep disorders, IBS, somatization disorders, or phobias.
Serotonin-associated disease states
Correlating with delta waves in the brain, serotonin affects your ability to rest, regenerate, and find serenity. Adequate serotonin allows the brain to recharge and rebalance itself each night, so that you can begin each morning with a fresh start. Serotonin is produced in the occipital lobes, which is also the center of sight.
As serotonin levels drop, the right and left hemispheres become desynchronized, producing feelings of being out of control. Moderately low levels can produce depression, mild hypertension, arthritis, poor temperature regulation, sexual disturbances such as premature ejaculation or delayed arousal response, bowel disturbances, mild PMS with emotional outbursts, learning disorders, obsessive- compulsive behavior, and insomnia, which tends to further lower serotonin levels. As levels drop further, hypertension can become uncontrolled, arthritis can intensify, PMS can become severe, and a wide range of perimenopausal symptoms can occur. With a severe shortage of serotonin, physical and psychological disturbances may become life threatening, with bingeing, masochism, severe depression and other serious mood disorders, addictions including alcoholism and drug abuse, somatization disorders, schizoaffective disorders, and schizophrenia with hallucinations. Physically, a severe serotonin deficiency can cause insomnia/ hypersomnia sleep cycles measured in days and increase hypertension to the point of producing a stroke.
Beyond detecting and treating frank disease states associated with serotonin deficiencies, physicians can analyze the balance of the four neurotransmitters to determine a patient’s personality type.
The serotonin-dominant personality
People with high serotonin levels (about 17% of the world’s population) know how to live in the moment. Realistic and impulsive, they are highly responsive to sensory input. They’re active participants in life who thrive on change. They take their vacations at a different spot each year. They try new foods, new hobbies, and new friends, and they have a natural disdain for order, structure, and authority. They’re optimistic, cheerful, easygoing, and the life of the party. A serotonin-dominant person gravitates to trades or professions that offer a variety of tasks, an ever-changing environment, and interactions with different people. Their keen hand-eye coordination makes them well suited to using various tools to accomplish their tasks. Construction workers, truck drivers, military personnel, hairstylists, pilots, surgeons, chiropractors, movie stars, fashion models, photographers, and professional athletes likely owe their skills to ample serotonin levels. Preferred sports can include mountain climbing, hunting, skydiving, hang gliding, scuba diving — just about anything that offers a personal challenge along with a certain level of excitement. They play hard and have the time of their life when doing activities that others would consider too dangerous. In relationships, they can be romantic and passionate, but they also love their independence and often refuse to be tied down. Due to their impulsivity and desire for change, they tend to move away from people before deep relationships develop. In fact, their friendships are typically many and varied — wide instead of deep. They have a fondness for children, but make better aunts and uncles than parents.
As with the other neurotransmitters, it is possible to have too much. An excess of serotonin can make a person extremely nervous. He can become hesitant, distracted, hypersensitive to criticism, and morbidly afraid of being disliked. Excessive serotonin can make a person believe he is inadequate and inferior. Sadness and anger are constant companions, and although he may have a desperate desire for interpersonal interaction, he is too fearful to even make an attempt.
The serotonin-deficient personality
Serotonin deficiency can occur from experiencing too much excitement (thereby metabolizing large amounts of serotonin) and/or not getting sufficient sleep (causing the brain to generate less serotonin). Shifts in personality occur at a much milder deficiency than the disease- producing deficiencies mentioned earlier. Personality shifts can, in fact, manifest when the serotonin level is only slightly lower than the levels of the other three neurotransmitters. And remember, we’re looking at the relative balance of neurotransmitters. A deficiency in one is usually offset by an excess of another, which typically produces the personality traits associated with a dominance of that other neurotransmitter.
A common sign of serotonin deficiency is depression and fatigue. The chronic lack of sufficient sleep means that the brain is unable to rest, regenerate, and resynchronize. This can manifest in the personality as a flat affect (a classic sign of depression) and a lack of pleasure, artistic appreciation, and common sense. The person may become codependent, obsessive- compulsive, or exhibit loner tendencies. He can be impulsive or perfectionistic, painfully shy or masochistic. Someone with multiple phobias is typically serotonin deficient. The frequent use of ecstasy, PCP, and LSD also signals a serotonin deficiency.
Lettin’ the good guys in,
Keepin’ the bad guys out
We have been made with a wonderful mechanism to prevent harmful substances from entering the brain. Not everything that circulates in the blood stream is allowed entry into the brain. There is a barrier between the blood and the brain, logically called the blood-brain barrier, that allows only glucose and certain nutrients selective access to the brain. This membrane protects the brain from toxins and other substances that would cause it damage. It also “holds in” certain substances manufactured by the brain, notably neurotransmitters, that would be lost through diffusion throughout the rest of the body if allowed to pass into the blood stream. Therefore, the same membrane that prevents toxins from passing through also prevents neurotransmitters from passing through. This characteristic of the blood-brain barier is the reason why a Parkinson disease patient, for example, cannot receive an injection of dopamine to restore the dopamine level in his brain and reverse the disease. So the dilemma is how to raise the level of specific neurotransmitters in the brain, when simple supplementation with those neurotransmitters is ineffective.
The answer lies in finding a way to “coax” the brain to produce more endogenous neurotransmitters. It turns out that the answer is fairly simple — give the brain more raw material, and it will make more neurotransmitters. Fortunately, the mechanism by which the brain makes each neurotransmitter is well known. Like most substances in the body, they are made through a series of chemical reactions. Notice that I said the blood-brain barrier allows only glucose and certain nutrients selective access to the brain. It is those “certain nutrients” that the brain uses to make neurotransmitters. If there is a deficiency in any of the nutrients needed to make a specific neurotransmitter, there will be a corresponding deficiency of that neurotransmitter. Supplementing the deficient nutrient(s) will allow the brain to resume full production of the neurotransmitter.
Building a better brain
So what are the “certain nutrients” that the brain must have? Without going into the chemistry of neurotransmitter manufacture, suffice it to say that the brain’s supply of amino acids is the most common limiting step in their production. Amino acids, the basic building blocks of protein, are also the basic raw material the brain uses to function. As such, they easily cross the blood-brain barrier. All amino acids can cross the blood-brain barrrier, in fact, but not all are used to make neurotransmitters. The problem is that all the amino acids circulating in the blood stream at any given time compete for passage through the “amino acid channels” in the blood-brain barrier, and passage of a specific amino acid is granted in proportion to its concentration in the blood. If you eat a steak or other complete protein source, all 20 amino acids are simultaneously competing for entry into the brain. Supplementing with, say, 1 gram of a certain amino acid won’t do much if you chase it with a glass of milk (15 grams of protein in 12 oz.) or take it with a meal. To be effective, amino acid supplements should be taken on an empty stomach with plain water or fruit juice (the fructose in juice helps escort the amino acid to the brain).
In the paragraphs that follow, I will tell you which amino acids are used to boost which neurotransmitter, and the primary food sources for that amino acid. Food sources are complex, however, and foods that boost the production of one neurotransmitter can also contain substances that boost the production of another. Eggs, for example, provide a tremenous boost for acetylcholine, but they also have a component that supports GABA. This is one reason why a change of diet takes longer to produce an effect than supplementation with pure amino acids. You should know that prescription drugs are also available to boost the production of a specific neurotransmitter or slow its destruction, but that is beyond the scope of this article. They are listed in detail in the reference given at the end of the article. (Note: numbers shown after the supplements listed below refer to the relative efficacy in boosting the neurotransmitter, on a scale of [1]=best to [4]=least effective.)
Boosting acetylcholine
- Pure amino acid precursors: serine, carnitine.
- Amino acid-boosting supplements: DMAE (dimethylaminoethanol) [1], phosphatidylcholine [1], phosphatidylserine [2], acetyl-L-carnitine [2], GPC (glycerol phosphocholine) [3].
- Supporting supplements: huperzine A [1], nicotine [1], lipoic acid (alpha-lipoic acid) [3], fish oils [3], manganese [4], conjugated linoleic acid [4].
- Hormonal supplements: DHEA (dehydroepiandrosterone) [2].
- Illegal supplements: LSD, PCP, psychotropic mushrooms.
- Dietary support: choline-rich foods, including avocado, cucumber, zucchini, lettuce, most fruit, bacon, bologna, hot dogs, chicken, turkey, pork, liver, fish, beef, milk, ice cream, sour cream, yogurt, cheese, eggs, and various nuts.
- Lifestyle support: aerobic exercise.
Boosting dopamine
- Pure amino acid precursors: phenylalanine, tyrosine.
- Amino acid-boosting supplements: N-acetyl tyrosine [2], L-tyrosine [3], phenylalanine [3]. (Note: most ingested phenylalanine is hydroxylated to tyrosine in the body. Tyrosine supplements, therefore, need one less chemical conversion step to be used by the body.)
- Supporting supplements: caffeine [1], guarana [1], yohimbe [1], ephedra[2], nicotine [2], Rhodiola rosea[3], thiamine [4], chromium [4], folic acid [4].
- Hormonal supplements: DHEA [2].
- Illegal supplements: cocaine, ecstasy, mescaline.
- Dietary support: phenylalanine- and tyrosine-rich foods, including wild game, duck, turkey, pork, chicken, luncheon meats, cottage cheese, ricotta, milk, yogurt, walnuts, soybeans, wheat germ, granola, rolled oats, dark chocolate, and eggs.
- Lifestyle support: sexual activity (for women), weight-bearing exercise, aerobic exercise.
Boosting GABA
- Pure amino acid precursor: glutamine.
- Amino acid-boosting supplements: L-glutamine [1].
- Supporting supplements: inositol [1], alcohol [1], B vitamins [2], glycine [3], kava [3], BCAA (branched-chain amino acids) [4], taurine [4].
- Hormonal supplements: progesterone [2].
- Illegal supplements: opioids, ketamine, marijuana, quaaludes.
- Dietary support: glutamine-rich foods (especially complex carbohydrates), including almonds, walnuts, and other tree nuts, whole-grain wheat and oats, rice bran, brown rice, lentils, potatoes, broccoli, spinach, bananas, citrus fruit, halibut, and beef liver.
- Lifestyle support: sexual activity (for men and women), sleep, aerobic exercise.
Boosting serotonin
- Pure amino acid precursor: tryptophan.
- Amino acid-boosting supplements: L-tryptophan [2], 5-HTP (5-hydroxytryptophan) [3].
- Supporting supplements: St. John’s wort [2], vitamin B6 [4], fish oils [4].
- Hormonal supplements: melatonin [1], progesterone [2].
- Illegal supplements: LSD, PCP, GHB, ecstasy.
- Dietary support: tryptophan-rich foods, including wild game, pork, luncheon meats, duck, turkey, chicken, wheat germ, cottage cheese, and eggs.
- Lifestyle support: aerobic exercise, psychotherapy, sleep.
To learn more
This series of articles is a synopsis of the groundbreaking research of Eric R. Braverman, MD, as presented at the American Academy of Anti-Aging Medicine (A4M) Annual Conference, June 2003. Dr. Braverman was a member of the pioneering research team at Havard University that developed the BEAM (Brain Electrical Activity Map), a noninvasive device to measure neurotransmitter levels in functioning brains through electrical activity. For more information, his book, The Edge Effect, is highly recommended reading.
Low Zinc / B6
Takeaway: If you're low in zinc, you will not have enough GABA to combat excess levels of norepinephrine. And if you are low in B6, you are likely to have problems with the same neurotransmitter.
The Importance of Zinc

The human body absorbs approximately 400kg zinc over the average 70-year lifespan and at any one time there should be 2-4 gm zinc in the body. It is the second most abundant mineral ion ( Magnesium is the first) in the body and is the only metal that appears in all enzyme classes The body absorbs 20-40% of zinc in food, zinc from animal foods being more readily absorbed (twice as much ) than zinc from plant foods. Zinc is also more readily absorbed with a protein meal and although the body cannot store zinc and it is needed every day in small amounts (50mg or less), it may be held in metallothionine reserves and transferred in metal transporter proteins. Metallothionines in the intestinal cells are capable of adjusting the absorption of zinc by 15-40%. Thus control of cellular zinc homeostasis is maintained by zinc proteins and zinc binding metallothioneines. Zinc is needed for over 300 enzymes in the body and makes up part of 3000 different proteins in the body. Muscles (60%) and bones (30%) contain 90% of the body’s zinc. High concentrations of zinc are found in the prostate gland and semen and the choroid of the eye.
If bone is reabsorbed or muscle is broken down then some zinc can be reutilised and in cases of zinc depletion changes in immune status alter before any decrease in levels of plasma zinc. There is a small exchangeable pool of zinc (100-200mg ) that depends on recently absorbed zinc and the intestinal excretion of zinc. As with Magnesium, the efficiency of absorption of zinc is inversely related to the amount of zinc present in the body. The greater the level of body zinc, the less absorption occurs. Zinc, Magnesium Calcium and Iron all compete for transporters in the intestine for uptake above a threshold of approximately 800mg so consuming these minerals together below this level should not interfere with uptake Zinc is found in all cells in the body and the daily requirement is dependent on age and activity.
Zinc deficiency is due to
Soil deficiency.
Some drugs deplete zinc.
Vegetarian and vegan diets may be deficient.
High cereal based diets, containing high phytate foods which can bind with zinc and impair absorption.
Cooking with water can result in leaching of up to 50% of zinc levels of the food.
Refined processing of wheat and baked goods can result in up to 75% zinc loss
Tetracycline and quinolone antibiotics react with zinc in the intestines inhibiting the absorption of both the antibiotic and zinc. The antibiotic should be taken 2 hours or more before or at least 4-6 hours after the zinc supplement to avoid this.
In short over 300 enzymes are zinc dependent, including enzymes involved in the synthesis of certain proteins such as collagen and wound healing. Also needed for thymic hormone activation and maintaining a normal immune system, testosterone and oestrogen, fertility and reproduction including cell division. It is involved in gene regulation, maintaining acid/base balance in the body and normal carbohydrate, fat and protein metabolism. It is needed for normal bones, skin, hair and nails and normal brain function including maintenance of normal vision. It can also act as an antioxidant, protecting DNA, lipids and proteins in the body.
Zinc Contributes to
Normal DNA synthesis. Although the exact role of zinc in DNA synthesis is not fully understood but it does play a structural role in zinc fingers, which are finger shaped proteins. Due to their shape, these proteins can bind to DNA and RNA allowing them to function in Gene expression. These proteins are the most common transcription factors in living organisms, transcription factors are proteins that bind to DNA and control the transfer of genetic information to RNA Put simply Zinc is needed for reading genetic instructions and lack of zinc may mean that instructions get misread or not read at all.
Normal acid/base metabolism. Acid/Base balance is the balance between acid and alkaline to keep body fluids as close to a neutral pH (pH7) as possible. Carbon dioxide and water are rapidly converted to bicarbonate and water (and back again) to maintain acid base balance in the blood and other tissues. The enzyme responsible for this is the zinc dependent enzyme Carbonic Anhydrase. Studies have shown that dietary deficiency of zinc reduces red blood cell carbonic anhydrase activity
Normal carbohydrate metabolism. Deficiency of zinc results in a drop of metabolic rate. Zinc dependent messenger RNA is needed to synthesise the enzymes required for carbohydrate metabolism so zinc deficiency may result in lack of these enzymes. Zinc may also interact with insulin by controlling the uptake of glucose by adipocytes (fat cells). Zinc deficiency results in impaired carbohydrate metabolism.
Normal cognitive function Zinc is highly concentrated in the cerebral cortex, pineal gland and hippocampus and zinc deficiency is associated with impaired memory formation and mood disorders. In the hippocampus zinc can reach concentrations of 8% of the total brain zinc. Zinc ions are also NDMA (N-methyl-D –aspartate) antagonists (NDMAs control memory function and excessive NDMA activation results in cell death due to excess calcium influx into neuronal cells ) so zinc becomes important for normal neuronal function and memory and delaying brain cell death . Normal fertility and reproduction. Steroid hormones such as testosterone and oestrogen are derived from cholesterol and zinc plays an important role in cholesterol metabolism. Low dietary zinc is associated with low concentrations of several hormones including testosterone.
Testosterone. Circulating testosterone and free testosterone appears to increase with oral zinc intake. In one study supplementing with 250 mg zinc sulphate for 6 weeks increased testosterone by 85% in people on hemodialysis.
Free Testosterone is converted to DHT (dehydrotestosterone) by the enzyme 5alpha-reductase ) primarily in the prostate gland, testes , adrenal glands and hair follicles. DHT is increased in infertile men and as it has an affinity for the hair follicles can result in male pattern baldness. Zinc has been shown to inhibit ( up to 98%)the enzyme 5 alpha reductase.
Semen: Semen is very rich in zinc. Sperm count, motility and physical characteristics of sperm increase and improve with some groups of infertile men.
Zinc deficiency has also been associated with increased expression of oestrogen receptors. The enzyme aromatase converts testosterone to oestrogen and zinc decreases aromatase activity so preventing excessive conversion of testosterone to oestrogen. Zinc deficiency can cause testicular cell death, increase protein oxidation in the testes, dysregulating other enzymes and proteins resulting in degeneration of testicular structures and impaired testosterone secretion.
Why should I Take A Zinc Supplement?
Normal macronutrient metabolism. Macronutrients are carbohydrates, fats and proteins. Zinc is needed for the enzymes that metabolise carbohydrates, fats and proteins
Normal metabolism of fatty acids- zinc is needed for the conversion of linoleic acid to Gamma Linolenic acid (GLA) and for the synthesis of prostaglandins series 1 ( Anti inflammatory prostaglandins) Zinc also plays an essential role in maintaining a balance between to different forms of prostaglandins.
Maintenance of normal serum testosterone concentrations, so involved in fertility and reproduction. Zinc plays a role in cell signalling, influencing hormone release and nerve function.
Normal metabolism of vitamin A. Zinc is necessary to maintain normal concentrations of vitamin A in the plasma, being essential for normal mobilization of Vitamin A from the liver. Zinc deficiency decreases the synthesis of Retinol Binding protein (RBP) in the liver leading to lower levels of RBP in the plasma.It influences the absorption, transport and utilisation of Vitamin A. . Zinc is also required for the enzyme Alcohol dehydrogenase , responsible for converting retinol to retinal, essential for eye function.
Normal protein synthesis. One of the important zinc dependent proteins is Gustin which is involved in taste and smell. Poor or absent gustin levels results in impaired taste and smell. Other important zinc containing enzymes are carboxopeptidase which helps break down protein. Zinc deficiency also impairs the synthesis of the protein Opsin, the precursor of Rhodopsin, which if decreased, results in abnormal dark adaptation of the eye. Zinc is also required for the enzyme alcohol dehydrogenase , responsible for converting retinol to retinal, essential for eye function. Haemoglobin is a protein and zinc s important in haemoglobin synthesis.
Maintenance of normal bones. Zinc regulates the secretion of calcitonin from the thyroid gland and therefore influences bone turnover. Zinc appears to regulate the bone matrix calcification in osteoblasts. Zinc deficiency decreases the activity of matrix proteins, type 1 collagen and alkaline phosphatase decreasing Calcium and Phosphorus accumulation. Therefore zinc deficiency may become a risk factor for poor extra cellular matrix calcification.
Maintenance of normal hair and nails Zinc is needed for building keratin and formation of collagen and for facilitating cell division that makes hair growth possible.
Maintainance of normal skin. Collagen in skin is produced by zinc dependent enzymes , the collagenases. Type 1 collagen is produced in the skin and is a structural long lived protein produced by fibroblasts. Collagen constitutes 70% skin mass and give the skin its structure and resistance to traction and strains. Total collagen decreases 1% a year resulting in decreased elasticity and aging skin. Zinc is essential not only for the enzymes producing collagen but also the cross linking that give collagen its stability. Human studies have shown that decreased zinc resulted in decreased total collagen.
Maintenance of normal vision Zinc supplementation alone significantly reduced the risks of developing AMD in subjects at higher risk. Zinc deficiency also impairs the synthesis of the protein Opsin, the precursor of Rhodopsin, which if decreased, results in abnormal dark adaptation of the eye. Zinc is also required for the enzyme alcohol dehydrogenase , responsible for converting retinol to retinal, essential for eye function.
Contributes to normal function of the immune system. Plays a central role in the immune system affecting cellular and humoral immunity. It is essential for thymic dependent T cells . Zinc deficiency results in decreased levels of all types of white blood cells. It is also required for the production of Thymulin (thymic hormone) Zinc ions also exhibit direct anti microbial activity.
Contributes to protecting the cells from oxidative damage, protecting the DNA, lipids and proteins . Loss of zinc from biological membranes increases their susceptibility to oxidative damage. Zinc is also necessary for the antioxidant enzyme Super Oxide Dismutase (SOD)and low levels of zinc supplementation resulted in increased levels of glutathione peroxidase , SOD and decreased lipid peroxidation.
The process of cell division. Zinc contributes to normal DNA synthesis and cell division. Zinc appears to be essential for Insulin like growth factor (IGF) which induces cell proliferation. Reduced zinc availability appears to affect membrane signalling and secondary messengers that coordinate cell proliferation. Ref : The Role of Zinc in Growth and Cell Proliferation by Ruth MacDonald published In The American Society for Nutritional Sciences Reference
What Are The Symptoms Of A Mild Zinc Deficiency?
Loss of appetite.
Poor growth.
Weight loss.
Diminished taste or smell.
Poor wound healing.
Skin problems, acne, psoriasis atopic dermatitis.
Poor vision, night blindness.
White spots on finger nails.
Depression, apathy.
What Are The Symptoms Of A Severe Zinc Deficiency?
Delayed sexual and bone maturation
Skin lesions
Diarrhoea
Loss of appetite
Hair loss
Increased susceptibility to infections
Behavioural changes
The passage of zinc into the body
Studies involving direct comparison of bioavailability of different forms of zinc in humans are few. The important fact is that the form of zinc needs to become dissociated into zinc ions which then bind to ligands ( proteins ) that transport the zinc into the cells of the small intestine. There are specific transport proteins that carry zinc across the cell membrane into the portal circulation where it is transported directly to the liver before being released into the circulation for delivery to all tissues. Approximately 70% of zinc is bound to serum albumin ( a plasma protein ) and factors altering serum albumin in turn affect serum zinc levels. Serum zinc has a rapid turnover to meet tissue demands.
Zinc is lost through the skin and kidneys (combined loss of 0.5-0.8mg/day) , more zinc being lost when the body sweats more, as in hot climates and during strenuous exercise. Approximately half of all zinc eliminated from the body is lost through the shedding of epithelial cells in the gastro intestinal tract (0.5- 3mg/day) and although a considerable amount is secreted through both biliary and intestinal secretions, most of the secretions are reabsorbed regulating the zinc balance. Starvation and muscle breakdown also increase zinc loss through the urine.
As already mentioned, protein enhances the absorption of zinc and a phytate rich diet (from cereals, grains, corn and rice) inhibit the absorption of zinc.
There is a very fine balance between zinc and copper. Zinc reduces the amount of copper your body absorbs because copper competes with zinc to bind with metallothionein, the binding protein that brings zinc into the intestinal cells. The ratio of zinc : copper is arguably more important than the concentration of either copper or zinc, a common problem being excessive copper in water from copper pipes or copper cookware.
Zinc also competes with iron to bind with blood transferring, illustrating the importance of a balance of these minerals. The ECRDA for zinc is 10 mg less is required for babies, children and teenagers and more for pregnant and breastfeeding ladies.
Recommended Daily Allowance For Zinc Supplements

Bioavailability Of Different Forms Of Zinc Supplements
There are many forms of zinc compounds.
Zinc Picolinate 20%
Zinc Ascorbate 15%
Zinc Chloride 48%
Zinc Sulphate 22%
Zinc Carbonate 52%
Zinc Citrate 31%
Zinc Bisglycinate 25%
There is not much substantial evidence of greater effectivity of one form of zinc over another as absorption of zinc in the body is subject to so many variables.
However, a small research study (15 healthy young adults in a randomised, double blind three way cross over study, receiving 10mg of elemental zinc as a supplement without food just published (20 November 2013) found that the bioavailability of zinc citrate was 61.3% , of zinc gluconate was 60.9% and of zinc oxide was 49.9 % Previous zinc intake may affect zinc bioavailability studies. Variables include;
Existing zinc status of the individual. The lower the zinc status of the individual, the greater the absorption of zinc.
People that sweat a lot are subject to more zinc loss, for example athletes, those in hot climate, menopausal ladies experiencing night sweats.
Dosage of zinc- as zinc intake in dosages is increased , percentage absorption decreases probably due to the saturation of the transport mechanisms.
Zinc absorption appears to be decreased in the elderly.
Zinc absorption is increased with dietary protein intake.
The type of protein in a meal affects zinc bioavailability. Animal protein enhances absorption.
Phytates in cereals and soy inhibit absorption of zinc by binding with it ( except zinc bisglycinate found in Metabolics zinc formula).
Caesin in milk and calcium inhibit absorption by binding with zinc ions.
Iron inhibits absorption of zinc.
Copper ( in high amounts ) inhibits Zinc absorption. In studies using 15mg zinc combined with 2mg copper no inhibition of absorption was found.
Cadmium- toxic levels of cadmium can inhibit zinc absorption
Conclusion
Types of zinc supplements may remain a personal preference, although generally zinc should not be taken on an empty stomach (as it can result in nausea) should be taken with an animal protein meal , away from cereals and taken in conservative doses to increase absorption. Long term zinc intake is recommended with copper (see zinc formula) as this is zinc bisglycinate, the only form not affected by phytates and balanced with a small amount of copper.
Enter coupon code: SSSCZinc to save 10%

Resistance Training’s Effect on Endurance Performance

Research shows that the appropriate integration of resistance training into the endurance athlete’s training can result in significantly better performance when compared to classic endurance training plans that focus only on aerobic endurance.
The following is an exclusive excerpt from the book Developing Speed, part of the NSCA’s Science of Strength and Conditioning Series with Human Kinetics.
Endurance athletes who are stronger can generally perform at a much higher level.
This suggests that training modalities that stimulate increases in muscular strength without compromising endurance capacity may be beneficial for the endurance athlete. Support for this contention can be found in the scientific literature; research shows that the appropriate integration of resistance training into the endurance athlete’s training plan can result in significantly better performance when compared to classic endurance training plans that focus only on aerobic endurance training.
When looking closely at endurance performance, several key factors—including the athlete’s maximal aerobic power (V˙ O2max), lactate threshold, and movement efficiency—contribute to performance (see figure 7.1). The training modality selected influences these factors by inducing changes to the athlete’s aerobic power and capacity, anaerobic capabilities, and neuromuscular function.

Aerobic training exerts a strong influence on both aerobic power and capacity, but it does not exert a great impact on the athlete’s anaerobic or neuromuscular abilities.
Conversely, resistance training exerts a strong influence on the athlete’s neuromuscular function and a moderate influence on anaerobic power and capacity, while offering only a minimal influence on aerobic power and capacity. By influencing the athlete’s anaerobic abilities as well as neuromuscular function, resistance training can elevate the athlete’s lactate threshold, movement efficiency, and ability to engage in high-intensity activities.
The ability of resistance training to improve endurance performance is likely related to several key factors, including the specific physiological and mechanical adaptations that are stimulated by the resistance training regimen. The integration of resistance training into the overall training plan appears to be central to creating these specific performance-enhancing adaptations.
Traditionally, endurance athletes and coaches have believed that resistance training either does not affect or negatively affects endurance performance. However, this view may be partially explained by a design flaw in many of the training programs that include both resistance and endurance training. The flaw is that resistance training is simply added to the endurance training plan. Athletes who undertake this approach often experience excessively high levels of fatigue that can negatively affect overall performance.
If athletes reduce their endurance training load to account for the addition of resistance training, then resistance training has a positive effect on the athletes’ endurance performance. The athlete who performs both resistance and endurance training in an integrated and appropriately planned fashion will perform at a higher level than the athlete who performs only classic endurance training.
Understanding Methylation
Methylation is a key biochemical process that is essential for the proper function of almost all of your body’s systems. It occurs billions of times every second; it helps repair your DNA on a daily basis; it controls homocysteine (an unhealthy compound that can damage blood vessels); it helps recycle molecules needed for detoxification; and it helps maintain mood and keep inflammation in check.
To keep methylation running smoothly you need optimal levels of B vitamins. Without enough B vitamins methylation breaks down, and the results can be catastrophic. In these cases we see more birth defects like spina bifida, more cases of Down’s syndrome, and more miscarriage.
A breakdown in methylation also puts you at higher risk for conditions like osteoporosis, diabetes, cervical dysplasia and cancer, colon cancer, lung cancer, depression, pediatric cognitive dysfunction ( mood and other behavioral disorders), dementia, stroke and may put you at a higher risk of heart disease.
To avoid all of these problems, the key is to maximize methylation. That means avoiding the things that cause your methylation to break down, testing to find out how well your methylation is working, and including the things that support proper methylation. Let’s look at how to do that.
8 Factors that Affect Your Methylation Process
- Genetics – Like an estimated 20 percent of us, you could be genetically predisposed to high homocysteine
- Poor diet – The word “folate” comes from “foliage.” You need to eat plenty of leafy greens, beans, fruit, and whole grains to get adequate levels of vitamins B6 and B12, betaine, and folate. Egg yolks, meat, liver, and oily fish are the main dietary sources of vitamin B12 — so long-term vegan diets can be a problem. Plus, certain compounds can raise levels of homocysteine and deplete the B vitamins. These include excess animal protein, sugar, saturated fat, coffee, and alcohol. Irradiation of food depletes nutrients, so foods treated this way may be lower in B vitamins, too
- Smoking – The carbon monoxide from cigarette smoke inactivates vitamin B6
- Malabsorption – Conditions like digestive diseases, food allergies, and even aging can reduce absorption of nutrients
- Decreased stomach acid – Aging and other conditions can reduce stomach acid — and therefore absorption of vitamin B12
- Medications – Drugs like acid blockers, methotrexate (for cancer and arthritis and other autoimmune diseases), oral contraceptives, HCTZ (for high blood pressure), and Dilantin (for seizures) can all affect levels of B vitamins
- Other conditions – These include hypothyroidism, kidney failure or having only one kidney, cancer, and pregnancy
- Toxic exposures – Some toxins can interfere with vitamin production
Watch out for these factors and you will go a long way toward protecting your methylation.
Measuring Your Own Methylation Process
To find out if your methylation process is optimal, ask your doctor for the following tests:
- Complete blood count – Large red blood cells or anemia can be a sign of poor methylation. Red blood cells with a mean corpuscular volume (MCV) greater than 95 can signal a methylation problem
- Homocysteine – This is one of the most important tests you can ask for. The normal level is less than 13, but the ideal level is likely between 6 and 8
- Serum or urinary methylmalonic acid – This is a more specific test for vitamin B12 insufficiency. Your levels may be elevated even if you have a normal serum vitamin B12 or homocysteine level
- Specific urinary amino acids – These can be used to look for unusual metabolism disorders involving vitamins B6 or B12 or folate, which may not show up just by checking methylmalonic acid or homocysteine
12 Tips to Optimize Your Methylation Process
Just as there are many causes of poor methylation, there are lots of things that support its proper functioning. Here’s how to maximize methylation — and prevent conditions like heart disease, cancer, dementia, depression, and more.
- Eat more dark, leafy greens – You want to eat l cup a day of vegetables like bok choy, escarole, Swiss chard, kale, watercress, spinach, or dandelion, mustard, collard, or beet greens. These are among the most abundant sources of the nutrients needed for optimal methylation
- Get more Bs in your diet – Good food sources include sunflower seeds and wheat germ (vitamin B6); fish and eggs (vitamin B6 and B12); cheese (B12); beans and walnuts (vitamin B6 and folate); leafy dark green vegetables; asparagus, almonds, and whole grains (folate); and liver (all three)
- Minimize poor quality animal protein, sugar, and saturated fat – Animal protein directly increases homocysteine. Sugar and saturated fat deplete your body’s vitamin stores
- Avoid processed foods and canned foods – These are depleted in vitamins
- Avoid caffeine – Excess amounts can deplete your B vitamin levels
- Limit alcohol to 3 drinks a week – More than this can deplete your B vitamin levels
- Don’t smoke – As noted above, smoking inactivates vitamin B6
- Avoid medications that interfere with methylation – See notes on this above
- Keep the bacteria in your gut healthy – Take probiotic supplements and use other measures to make sure the bacteria in your gut are healthy so you can properly absorb the vitamins you do get
- Improve stomach acid – Use herbal digestives (bitters) or taking supplemental HCl
- Take supplements that prevent damage from homocysteine –Antioxidants protect you from homocysteine damage. Also make sure you support methylation with supplements like magnesium and zinc
- Supplement to help support proper homocysteine metabolism – Talk to your doctor to determine the best doses and forms for you. Here are a few suggestions:
Folate (folic acid): Amounts can vary based on individual needs from 200 mcg to 1 mg. Some people may also need to take preformed folate (folinic acid or 5 formylTHF) to bypass some of the steps in activating folic acid
Vitamin B6: Take 2 to 5 mg a day. Some people may need up to 250 mg or even special “active” B6 (pyridoxyl-5-phosphate) to achieve the greatest effect. Doses higher than 500 mg may cause nerve injury
Vitamin B12: Doses of 500 mcg may be needed to protect against heart disease. Oral vitamin B12 isn’t well absorbed; you may need up to 1 or 2 mg daily. Ask your doctor about B12 shots
Betaine: This amino acid derivative is needed in doses from 500 to 3,000 mg a day, depending on the person
Understanding Cholesterol
Cholesterol is one of the least understood molecules and truly gets a "bad rap." Although people understand that cholesterol is only present in animal-based foods, what many do not know is that we produce cholesterol just like any other animal, and it is a very necessary molecule used to form all of the cell membranes in the body. Cholesterol is also the building-block molecule from which all of the steroid hormones are made. If there is more cholesterol in the diet than is needed, then the body synthesizes less. If the diet does not provide enough cholesterol then the body makes more.
Since cholesterol is used by the body to manufacture hormones such as cortisol, we can look at what cortisol is and make some logical connections. Cortisol is widely regarded as a "stress hormone" since the body needs and produces more of it in response to stress. This stress response takes many forms; one of them is lowering inflammation--useful if your version of stress involves hand-to-hand combat with large carnivores or fighting for your life. The lowering of inflammation is why the pharmaceutical versions of cortisol (Hydrocortizone and other glucocorticoids) are used to reduce inflammation in cases of massive trauma or major surgery. Other effects of cortisol are the elevation of blood pressure, release of glucose from the liver, inhibition of the immune system, retaining of water/reducing kidney function (probably useful if the combat with the large carnivores leads to bleeding form flesh wounds, as retaining water would help to maintain blood volume when bleeding profusely) and other effects. Taken together, when stress levels remain high, lots of cortisol is produced. It would then make sense that making a lot of cortisol requires a lot of what is made from, which is cholesterol. Therefor, during periods of high stress (a lifetime for many people), the levels of cholesterol can become very elevated. When the stress is long-term, the stress will end up raising the inflammation level through other mechanisms; effectively, stress reduces inflammation in the short-term only. Cholesterol has many other uses in the body, including the formation of myelin--the insulating/speeding sheath that wraps around the nerves, like rubber coating surrounding a copper wire, that increases their conduction velocity (and is damaged in multiple sclerosis).
Dietary modifications to reduce cholesterol has been met with mixed results. Some people can follow a strict no-cholesterol diet and achieve a lowering of their plasma cholesterol levels, while other are not able to accomplish this. This failure of dietary regimen to achieve the desired goal may be because of the body's production of cholesterol to meet the necessary levels for the amount of stress the individual is experiencing. The failure may also be because of reduced utilization of cholesterol. The gut bacteria play a role here also with Lactobacillus bacteria actively consuming cholesterol. Lactobacillus not only consumes cholesterol, but it makes bile acids that aid in the digestion of fats out of the cholesterol that it consumes. It therefore makes sense that if a person has altered gut bacteria demographies and Lactobacillus are in the minority, that person will not use up as much cholesterol and the cholesterol levels may accumulate. Elevated levels of stress reduce the levels of Lactobacillus, providing the pathway for stress to reduce the beneficial effects of a healthy diet. The same imbalance may also predispose the person to inflammation, which is the real cause of heart disease.
The use of probiotics in dairy products to control cholesterol greatly predates modern science, as the Maasai tribe in Kenya use a probiotic fermented milk in their diet. The Maasai diet is composed almost entirely of meat, milk and blood. This diet includes several times the recommended level of cholesterol, and yet the Maasai have no problems with atherosclerosis or other degenerative diseases that could be related to their diet. What has been found is that their fermented milk (no refrigeration, so it all gets fermented if not immediately consumed!) contains probiotic bacterial population s that help to consume and lower cholesterol. Other sources of probiotics, such as yogurt, have been found to lower cholesterol levels also.
Many people incorporate yogurt into their diet because they like it or they think that it is healthy--but what makes it healthy? Much of the yogurt on store shelves has no bacterial colony whatsoever, so it is important to read the ingredients! If it has no "live active cultures," then it has little if any health benefit to our good bacteria and subsequent immune function.
Eggs have often been the poster child of high cholesterol food, if the yolk is used. However, consuming eggs may not have as much to do with elevated cholesterol level as initially thought. Similarly, fats were implicated in the disease process, as it has been observed that people with high triglycerides (fats) in their blood are at increased risk of developing heart disease. There are other variables in this equation, as is often the case. For example, abnormal populations of gut bacteria promote atherosclerosis by causing inflammatory changes and altered metabolism of lipids. The presence of abnormal gut bacteria that cause irritable bowel syndrome is directly linked to the development of thickening of the wall of arteries, which is of course the actual structural change that is at the center of what we call atherosclerosis.
Excerpt from The Symboint Factor by Richard Matthews DC DACNB FACFN
Healthcare: Treating the Symptoms and Not the Problem
We experience symptoms of illness (ie high blood pressure or dysbiosis) as a sign that something within the body is not working as it should. The presence of symptoms should alert a person that the body has become imbalanced in some way, so that action can be taken to restore balance and function. Instead, most people are taught to treat the symptoms only. Examples would be taking pain relievers to control pain or using muscle relaxers for muscle spasms or even blood pressure pills and statin drugs to help with risk factors for heart disease. This unfortunately does not correct the underlying imbalance that caused the dysfunction and symptom to result. The true problem may continue creating imbalances in the body's system until more serious conditions manifest.
There are few cases of "one cause, one cure" that happen in the human body. Pursuing health means maximizing the function of all the body's intrinsic systems as well as the brain. This is a completely different concept than what we usually encounter in healthcare. Often asked is the question: "will my insurance cover that?" when explaining health-building strategies, and the answer is almost always a "no." The reason is that insurance companies sell disease care policies, not health care policies. The number of pure health building interventions that are covered, if any, can often be counted on one hand. For example, does insurance cover nutritional supplements, gym memberships, yoga classes, new bicycles, probiotic foods, kitchen tools such as a VitaMix and similar items? Perhaps some of these are covered items in some countries, but not in the United States. Nothing that prevents cancer is covered, but annual early detection is, to see if your have it yet. The "system" is geared toward specific treatment for a specific disease, and yet almost all diseases have several factors or circumstances as causes. If a person falls and breaks a wrist, the doctor that treats that wrist has a very specific job. If the patient instead has arthritis and migraines, what are the causes? Inflammation, poor diet, biomechanical issues, lifestyle, genetics--four out of five of these are variables that we have control over and yet often do nothing about.
Adapted from The Symboint Factor by Richard Matthews DC DACNB FACFN
Avoid the Worst Ingredients
Flavor enhancers, preservatives, sweeteners, synthetic colors and manmade fats and chemicals commonly hide out in the ultra-processed foods we eat. If you want to stay away from putting harmful chemicals on your table, it’s necessary to learn how to identify the worst ingredients and find healthier alternatives. Let’s take a look at how to get started.
1. Identify and avoid these seriously dangerous additives
It’s not easy to remember all of the worst ingredients to steer clear of, but learning to avoid the most toxic ones commonly found in the food supply can drastically improve your health. A common food additive is monosodium glutamate (MSG) that is very dangerous and affects human body in a variety of ways. Headache, nausea, vomiting, pain in the back of the neck, numbness and heart palpitations are common side-effects of consuming MSG. Monosodium glutamate is an excitotoxin that overexcites the cells in your body to the extent where they are so heavily damaged that they die. MSG also leads to a range of neurological diseases on prolonged exposure. (1, 2)
It’s not easy to find processed foods that are completely free of MSG. Other food ingredients often mask the presence of MSG, including:
- autolyzed yeast
- hydrolyzed protein
- hydrolyzed vegetable protein
- sodium caseinate
- yeast nutrient or yeast extract
- Torulo yeast
- natural flavoring
- glutamic acid
Soy sauce, seasonings, powdered milk, stock, malt, maltodextrin, pectin and anything protein often contain MSG.
2. Avoid the toxic heart attack ingredient
Trans fats are very harmful. These artificial trans fatty acids lower the level of good cholesterol (HDL) and increase the level of bad cholesterol (LDL) in your body. Primarily used in processed foods, trans fats are formed when food manufacturers add hydrogen to liquid oil to solidify it. (They do this to increase shelf life.) Unfortunately, trans fats have been blamed for up to 50,000 premature heart attack deaths a year. (3)
In the hydrogenation process, oil is heated to an extremely high temperature of about 500 to 1000 degree Celsius. Hydrogenated oil is a fabulous preservative because all the natural enzymes are destroyed by the high heat, rendering the end product as an unhealthy sludge. If you see terms like hydrogenated oil, partially hydrogenated oil or fractionated oil on food label, do not buy the products.
3. Steer clear of metabolism-sinking sweeteners
Artificial sweeteners may seem like a good choice if you’re watching your calories, but science shows us it’s really one of the worst ingredients when it comes to your metabolic health. High-fructose corn syrup (HFCS) is a sweetener that leads to weight gain, heart complications and obesity.
Some artificial sweeteners result in headaches and mood swings as well. Aspartame, saccharin and sucralose are widely used artificial sweeteners and can exert a bigger load on your metabolic system than plain old sugar. They also trick your brain into feeling less full, prompting you to eat more, which in turn can lead to weight gain. So monitor your intake of artificial sweeteners to stay fit.
4. Beware of these 3-letter cancer causers
Butylated hydroxyanisole (BHA) and Butylated hydroxytoluene (BHT) are processed food preservatives that have been found to have carcinogenic properties by the International Agency for Research on Cancer. BHA has been declared safe by FDA, but it is termed ‘reasonably anticipated to be a human carcinogen’ by U.S. Department of Health and Human Services. (4, 5)
BHA has been shown to act as an endocrine disruptors, interfering with healthy hormone production, too. (6) BHA and BHT preservatives are commonly found in cereals, potato chips, chewing gum and cereal snack mixes. (Read your cosmetics labels, too. They often hide out in personal care products.)
5. Don’t assume soy is safer
Is soy bad for you? In the majority of cases, particularly as it pertains to soy as an ingredient in processed foods, it is unhealthy. While many of us think that soy and soy products as healthy and protein-rich, this is not always true. A majority of soy used in processed food products is genetically engineered. That means the crop has been tinkered with on a genetic level to receive applications of glyphosate, the main ingredient in Roundup weedkiller, without killing the plant. This has led to “excessive” levels of glyphosate turning up in the food we eat. (7) In 2015, the World Health Organization declared glyphosate “probably carcinogen to humans.” That makes conventional soy one of the worst ingredients.
Consuming GMO ingredients in considerable quantity over a long period of time is suspected to lead to infertility, gluten disorders, allergies and even cancer. Though the jury is still out on this controversial topic, with several studies showing that GMO ingredients are safe, I suggest practicing the precautionary principle, meaning it’s always best to consume processed foods that rely the least on GMO ingredients, staying as natural as possible. (8)
Factors in Non-Contact ACL Injuries
A short animation of typical conditions leading to a non-contact ACL injury.
Pre Workout Supplements: Hypertrophy Priority
Here are some supplement recommendations for athletes seeking to maximize Hypertrophy. With Hypertrophy we are trying to maximize the acidic environment to induce as much damage, cell swelling and hyperemia as possible. What can we take preworkout to help this along?
Primarily, we will want to look at things that shuttle nutrients and blood into the muscle.
- Citruline Malate: reduces fatigue and improves muscle endurance. More effective than Arginine. Arginine actually decreases GH during your workout when taken pre exercise. Arginine is best used before bed.
- Antioxidants : Alpha Lipoic Acid, grape seed extract and CoQ10 improve mitochondrial function and will allow for more blood flow to muscles during training.
- Beet Root Powder: Vasodilator, will induce a pretty gnarly pump.
- Neurotransmitter boosters: these will be important for anyone that has a hard time getting amped up to train. I advise against taking caffeine as a pre workout before Hypertrophy sessions because caffeine is a vaso constrictor. That means that taking caffeine with nutrients to chase the pump is a bit futile. There is a trade off for sure. If training without caffeine leads to a shit workout, then it may be worth your while to take caffeine instead of some of the vasodilators. Taking both at the same time though, to me, is a waste of money.
- BCAAs: provides energy and will prevent muscle protein breakdown during training.
- Creatine: will help sustain energy levels throughout your sessions and get more fluid into the muscles.

Why do partial squats not transfer very well to sport?
By Chris Beardsley, S&C Research columnist
Partial squats make you stronger at partial squats, but do not transfer to full squats. On the other hand, full squats make you stronger at full squats and also make you stronger at partial squats (although usually not quite as well as partial squats).
This is probably because the mechanisms that produce joint angle-specific strength gains are different after training at long muscle lengths, compared to training at short muscle lengths. Training at longer muscle lengths involves more regional hypertrophy, which seems to transfer better to strength across the whole range of motion.
Even so, many coaches have noted that the joint angles in partial squats are similar to the joint angles in the stance phase of running gait, or during jumping. Because of this similarity between joint angles, they suggest that partial squats should transfer better to sport than full squats, as they should produce the greatest gains in strength exactly where we need them.
And this makes a lot of sense.
On the other hand, most research shows that full squats are superior compared to partial squats for improving athletic performance in many respects, particularly jumping.
So what mechanism could be causing this disparity?
What is the background?
You should be able to follow this article without too many problems if you remember that we are normally stronger at one joint angle compared to all the rest, which we call the angle of peak torque.
This angle of peak torque can be changed in different ways, by different types of training.
Training programs using full ranges of motion, using long muscle lengths, or eccentrically all tend to move the angle of peak torque to a joint angle corresponding to a longer muscle-tendon length. In contrast, training programs using a partial range of motion, or short muscle lengths, tend to move the angle of peak torque to a joint angle corresponding to a shorter muscle-tendon length.
And most importantly, changing the angle of peak torque is very likely one of the main mechanisms that causes joint angle-specific gains in strength.
However, angles of peak torque are normally measured using isometric tests, and they might differ during dynamic contractions, particularly at higher speeds.
So does this happen?
Do angles of peak torque differ with angular velocity?
Full range of motion exercises might transfer better to sport than partial range of motion exercises if the angles of peak torque are different when we measure them at different speeds.
This will be particularly relevant if our exercises are traditional, heavy squats, as they involve much slower movement speeds than jumping or sprinting.
And this does happen!
The angle of peak torque is seen at joint angles corresponding to shorter muscle-tendon lengths as angular velocity increases (Moffroid et al. 1969; Knapik et al. 1983; Kannus & Jarvinen, 1991; Yoon et al. 1991; Khalaf et al. 1997; Khalaf et al. 2001; Khalaf & Parnianpour, 2001; Anderson et al. 2007; Ripamonti et al. 2008), although this effect is not always observed consistently in every study, and is much less marked above 180 degrees/s (Frey-Law et al. 2012).
The following charts derived from data reported by Yoon et al. (1991) show how the angle of peak torque alters with increasing angular velocity. Each line represents a different angular velocity moving through the same joint angle range of motion.
Here is knee flexion (contracting from left to right):

As you can see, as the movement speed increases, two things happen.
Firstly, the lines shift downwards, because force reduces as angular velocity increases (because of the force-velocity relationship).
Secondly, the angle of peak torque moves further to the right as angular velocity increases. This means that the angle of peak torque occurs at progressively shorter and shorter muscle-tendon lengths as angular velocity increases.
Here is knee extension (contracting from left to right):

Why do angles of peak torque differ with changing speed?
As you can see from the charts, the angle of peak torque moves to a joint angle that corresponds to shorter and shorter muscle-tendon lengths, with increasing speed.
This probably happens because even though the muscle-tendon lengths are the same at each joint angle, the muscle and tendon do not change length in the same way at different contraction speeds (don’t forget that tendons always lengthen to a greater or lesser extent when a muscle contracts, even when the contraction is purely a concentric contraction that involves a shortening of the muscle-tendon unit).
Fast contractions involve small muscle forces, which cause a smaller amount of tendon elongation at the start of the contraction.
The smaller amount of tendon elongation in fast contractions means that the muscle stays lengthened for longer in the concentric phase of the contraction. This allows the muscle to stay on the plateau of the length-tension curve for longer. Therefore, the angle of peak torque is shifted to much later in the overall joint angle range of motion (Murray et al. 1980).
Slow contractions involve high muscle forces, which cause much more tendon elongation at the start of the contraction.
This greater tendon elongation means that the muscle does not remain lengthened for very long during the concentric contraction. So it drops off the plateau of the length-tension curve quickly. Therefore, the angle of peak torque is seen earlier on in the overall joint angle range of motion (Murray et al. 1980). And isometric contractions are the slowest, strongest contractions of all.
Why is this important?
Why is contraction speed important for the angle of peak torque?
There are two key implications.
Firstly, it means that the angle of peak torque in dynamic movements is always at joint angles corresponding to shorter muscle-tendon lengths compared to the isometric angle of peak torque.
Secondly, it means that sporting movements at very high angular velocities have angles of peak torque at joint angles corresponding to very short muscle-tendon lengths. However, even when measured in the same person, these are not the same angles of peak torque as slower, barbell exercises or isometric tests. Those angles of peak torque occur at much longer muscle-tendon lengths.
This may be why full range of motion heavy resistance training exercises transfer better than similarly-loaded partial range of motion exercises to many high-velocity athletic movements.
What does this mean for jumping?
The quadriceps are key for jumping, and most jumping requires an angle of peak torque at moderate quadriceps lengths, as neither jumpers nor team sports athletes bend their knees down to the levels seen during a full squat before take-off.
This has led some coaches to assume that partial squats might be helpful, as they seem to involve a peak contraction around the same sort of joint angle.
But although this sounds logical, it ignores how the angle of peak torque changes with movement speed.
During a slow, heavy squat, the angle of peak torque will be observed at long muscle lengths. On the other hand, a jump is clearly a very fast movement and so the corresponding angle of peak torque will be at a much shorter muscle length.
If we train at long quadriceps muscle lengths, such as in the deep squat, we shift the angle of peak torque towards a longer muscle length. Because increasing movement speed moves angles of peak torques towards shorter muscle lengths, however, this will correspond to an angle of peak torque at moderate muscle lengths when we measure it at a fast velocity.
This is exactly where we need them for the jump.
If we train at short-to-moderate quadriceps muscle lengths, such as in the partial squat, we shift the angle of peak torque towards a shorter muscle length. Because increasing movement speed moves angles of peak torques towards shorter muscle lengths, however, this will correspond to an angle of peak torque at very short muscle lengths when we measure it at a fast velocity.
This is not where we want them for the jump.
And this is why deep squats transfer much better to jumping than partial squats (Weiss et al. 2000; Hartmann et al. 2012; Bloomquist et al. 2013).
Although there is less research available for sprinting, the same principles will apply.
Conclusions
Some people have proposed that partial squats should transfer better to sport than full squats because of the similar joint angles involved. However, full squats are definitely superior, and this is very clear in relation to jumping.
The reason for this discrepancy is that the angle of peak torque changes with movement speed. The angle of peak torque is found at shorter muscle-tendon lengths when measured at fast speeds, compared to when measured at slow speeds.
This is likely because even though the muscle-tendon lengths are the same at each joint angle, the muscle and tendon do not lengthen to the same extent at different speeds, and the amount of tendon elongation is less during fast contractions, which allows the muscle to remain on its length-tension plateau for longer.
Heavy, slow exercises such as full squats produce peak contractions at long muscle-tendon lengths. Because of differences in the amount that the tendon changes length, these angles of peak torque correspond very well to the peak contractions in athletic movements at joint angles corresponding to shorter muscle-tendon lengths, such as in jumping.
References
- Anderson, D. E., Madigan, M. L., & Nussbaum, M. A. (2007). Maximum voluntary joint torque as a function of joint angle and angular velocity: model development and application to the lower limb.Journal of Biomechanics, 40(14), 3105-3113.
- Bloomquist, K., Langberg, H., Karlsen, S., Madsgaard, S., Boesen, M., & Raastad, T. (2013). Effect of range of motion in heavy load squatting on muscle and tendon adaptations. European Journal of Applied Physiology, 113(8), 2133-2142.
- Frey-Law, L. A., Laake, A., Avin, K. G., Heitsman, J., Marler, T., & Abdel-Malek, K. (2012). Knee and elbow 3d strength surfaces: peak torque-angle-velocity relationships. Journal of Applied Biomechanics, 28(6), 726-737.
- Hartmann, H., Wirth, K., Klusemann, M., Dalic, J., Matuschek, C., & Schmidtbleicher, D. (2012). Influence of squatting depth on jumping performance. Journal of Strength & Conditioning Research, 26(12), 3243.
- Kannus, P., & Jarvinen, M. (1991). Knee Angles of Isokinetic Peak Torques in Normal and Unstable Knee Joints. Isokinetics and Exercise Science, 1(2), 92-98.
- Khalaf, K. A., Parnianpour, M., Sparto, P. J., & Simon, S. R. (1997). Modeling of functional trunk muscle performance: Interfacing ergonomics and spine rehabilitation in response to the ADA.Journal of Rehabilitation Research and Development, 34(4), 459.
- Khalaf, K. A., Parnianpour, M., & Karakostas, T. (2001). Three dimensional surface representation of knee and hip joint torque capability. Biomedical Engineering: Applications, Basis and Communications, 13(02), 53-65.
- Khalaf, K. A., & Parnianpour, M. (2001). A normative database of isokinetic upper-extremity joint strengths: towards the evaluation of dynamic human performance. Biomedical Engineering: Applications, Basis and Communications, 13(02), 79-92.
- Knapik, J. J., Wright, J. E., Mawdsley, R. H., & Braun, J. (1983). Isometric, isotonic, and isokinetic torque variations in four muscle groups through a range of joint motion. Physical Therapy, 63(6), 938-947.
- Moffroid, M., Whipple, R., Hofkosh, J., Lowman, E., & Thistle, H. (1969). A study of isokinetic exercise. Physical Therapy, 49(7), 735.
- Murray, M. P., Gardner, G. M., Mollinger, L. A., & Sepic, S. B. (1980). Strength of Isometric and isokinetic contractions knee muscles of men aged 20 to 86. Physical Therapy, 60(4), 412-419.
- Ripamonti, M., Colin, D., & Rahmani, A. (2008). Torque–velocity and power–velocity relationships during isokinetic trunk flexion and extension. Clinical Biomechanics, 5(23), 520-526.
- Weiss, L. W., Fry, A. C., Wodd, L. E., Relya, G. E., & Melton, C. (2000). Comparative Effects of Deep Versus Shallow Squat and Leg-Press Training on Vertical Jumping Ability and Related Factors. The Journal of Strength & Conditioning Research, 14(3), 241-247.
- Yoon, T. S., Park, D. S., Kang, S. W., Chun, S. I., & Shin, J. S. (1991). Isometric and isokinetic torque curves at the knee joint. Yonsei Medical Journal, 32(1), 33-43.